Center for Population Health Sciences, Center for Primary Care and Outcomes Research, and Departments of Medicine and of Health Research and Policy, Stanford University, Palo Alto, CA, USA; Center for Primary Care, Massachusetts General Hospital, Boston, MA, USA.
Division of General Medicine, University of Michigan, and Center for Clinical Management Research, Veterans Affairs Ann Arbor Healthcare, Ann Arbor, MI, USA.
Lancet Diabetes Endocrinol. 2017 Oct;5(10):788-798. doi: 10.1016/S2213-8587(17)30221-8. Epub 2017 Aug 10.
In view of substantial mis-estimation of risks of diabetes complications using existing equations, we sought to develop updated Risk Equations for Complications Of type 2 Diabetes (RECODe).
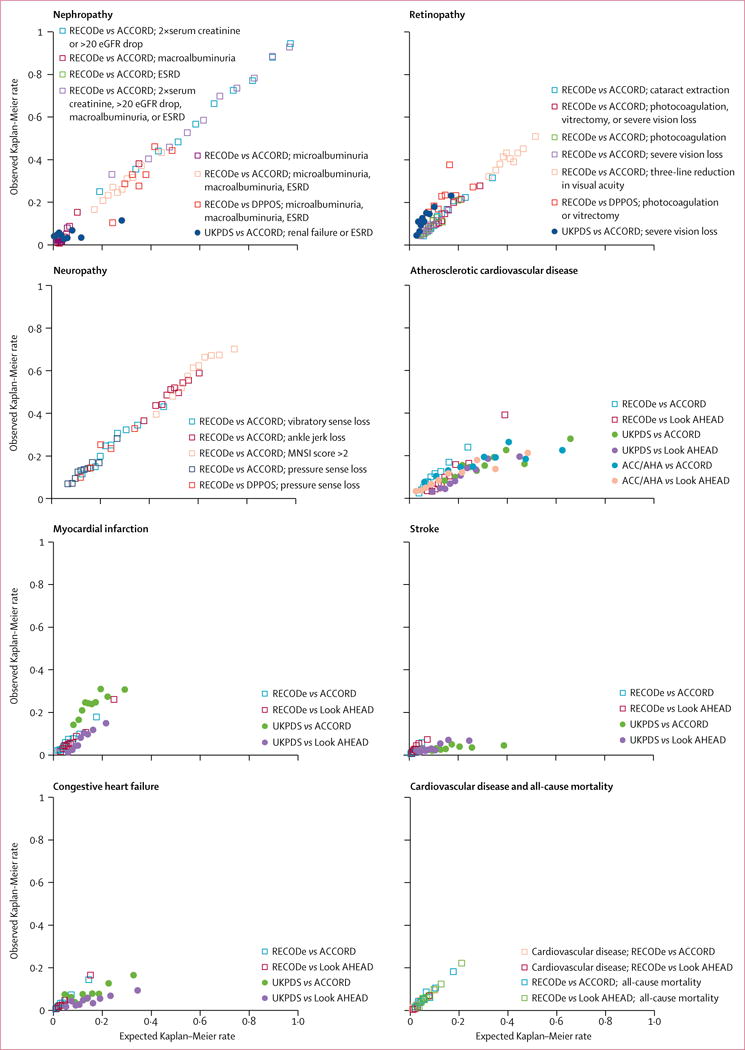
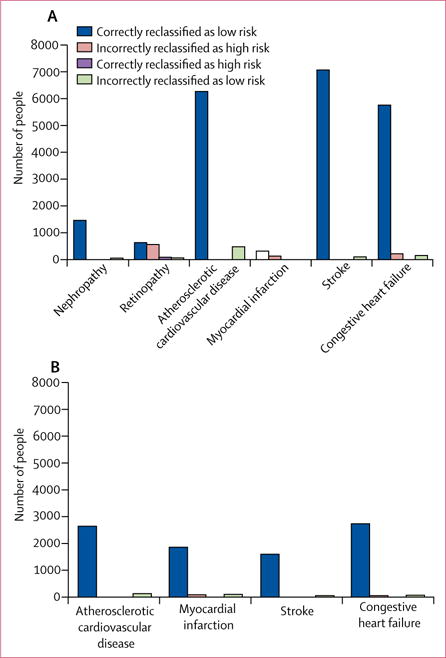
To develop and validate these risk equations, we used data from the Action to Control Cardiovascular Risk in Diabetes study (ACCORD, n=9635; 2001-09) and validated the equations for microvascular events using data from the Diabetes Prevention Program Outcomes Study (DPPOS, n=1018; 1996-2001), and for cardiovascular events using data from the Action for Health in Diabetes (Look AHEAD, n=4760; 2001-12). Microvascular outcomes were nephropathy, retinopathy, and neuropathy. Cardiovascular outcomes were myocardial infarction, stroke, congestive heart failure, and cardiovascular mortality. We also included all-cause mortality as an outcome. We used a cross-validating machine learning method to select predictor variables from demographic characteristics, clinical variables, comorbidities, medications, and biomarkers into Cox proportional hazards models for each outcome. The new equations were compared to older risk equations by assessing model discrimination, calibration, and the net reclassification index.
All equations had moderate internal and external discrimination (C-statistics 0·55-0·84 internally, 0·57-0·79 externally) and high internal and external calibration (slopes 0·71-1·31 between observed and estimated risk). Our equations had better discrimination and calibration than the UK Prospective Diabetes Study Outcomes Model 2 (for microvascular and cardiovascular outcomes, C-statistics 0·54-0·62, slopes 0·06-1·12) and the American College of Cardiology/American Heart Association Pooled Cohort Equations (for fatal or non-fatal myocardial infarction or stroke, C-statistics 0·61-0·66, slopes 0·30-0·39).
RECODe might improve estimation of risk of complications for patients with type 2 diabetes.
National Institute for Diabetes and Digestive and Kidney Disease, National Heart, Lung and Blood Institute, and National Institute on Minority Health and Health Disparities, National Institutes of Health, and US Department of Veterans Affairs.
鉴于现有方程对糖尿病并发症风险的严重估计错误,我们试图开发更新的 2 型糖尿病并发症风险方程(RECODe)。
为了开发和验证这些风险方程,我们使用了来自心血管风险控制行动中的糖尿病研究(ACCORD,n=9635;2001-09)的数据,并使用来自糖尿病预防计划结果研究(DPPOS,n=1018;1996-2001)的数据验证了微血管事件的方程,以及使用来自糖尿病行动研究(Look AHEAD,n=4760;2001-12)的数据验证了心血管事件的方程。微血管结果为肾病、视网膜病变和神经病变。心血管结果为心肌梗死、中风、充血性心力衰竭和心血管死亡率。我们还将全因死亡率作为一个结果纳入其中。我们使用交叉验证的机器学习方法,从人口统计学特征、临床变量、合并症、药物和生物标志物中选择预测变量,纳入每个结局的 Cox 比例风险模型。通过评估模型区分度、校准度和净重新分类指数,将新方程与旧风险方程进行比较。
所有方程的内部和外部区分度均为中等(内部 C 统计量为 0.55-0.84,外部 C 统计量为 0.57-0.79),内部和外部校准度均较高(观察到的和估计的风险之间的斜率为 0.71-1.31)。我们的方程在区分度和校准度方面优于英国前瞻性糖尿病研究结果模型 2(用于微血管和心血管结局,C 统计量为 0.54-0.62,斜率为 0.06-1.12)和美国心脏病学会/美国心脏协会队列方程(用于致命或非致命性心肌梗死或中风,C 统计量为 0.61-0.66,斜率为 0.30-0.39)。
RECODe 可能会改善 2 型糖尿病患者并发症风险的估计。
美国国立卫生研究院下属的国家糖尿病、消化和肾脏疾病研究所、国家心肺血液研究所和国家少数民族健康与健康差异研究所,以及美国退伍军人事务部。