Ide Akane, Amino Nobuyuki, Kudo Takumi, Yoshioka Waka, Hisakado Mako, Nishihara Eijun, Ito Mitsuru, Fukata Shuji, Nakamura Hirotoshi, Miyauchi Akira
Kuma Hospital, Centre for Excellence in Thyroid Care, 8-2-35 Shimoyamate-dori, Chuo-ku, Kobe, 650-0011 Japan.
Thyroid Res. 2017 Aug 8;10:4. doi: 10.1186/s13044-017-0039-0. eCollection 2017.
Pregnancy and delivery markedly influence thyroid function. However, the comparative prevalence of gestational thyrotoxicosis (GT), new onset of Graves' disease during pregnancy (GD during pregnancy), postpartum destructive thyrotoxicosis (PPT), and postpartum Graves' thyrotoxicosis (PPGD) has not yet been determined.
We prospectively registered and performed a review of 4127 consecutive non treated female patients with thyrotoxicosis, seen between August 2008 and December 2013 in our outpatient clinic of Kuma Hospital. 187 out of the 4127 women had new diagnosis of thyrotoxicosis during pregnancy or in the postpartum period. We investigated the prevalence of new diagnosis of GT, GD during pregnancy, PPT and PPGD and compared the characteristics of these types of thyrotoxicosis. The postpartum period is defined as twelve months after delivery.
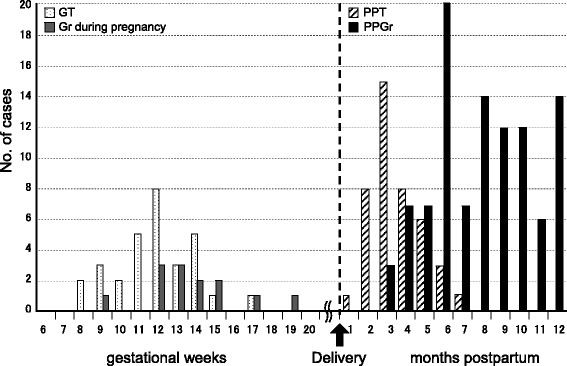
Out of 187 pregnant or postpartum women, we identified 30 (16.0%) with GT, 13 (7.0%) with GD during pregnancy, 42 (22.5%) with PPT, and 102 (54.5%) with PPGD. The onset time of thyrotoxicosis during pregnancy, i.e., both GT and GD during pregnancy, was delayed by a couple of weeks when hCG peaked at 10 gestational weeks. Seventy-six percent of patients with PPT developed thyrotoxicosis between delivery and 4 months postpartum; on the other hand, 83.3% of patients with PPGD developed thyrotoxicosis at 6 months postpartum or later.
We named gestational thyrotoxicosis, new onset of Graves' disease during pregnancy, postpartum destructive thyrotoxicosis, and postpartum Graves' thyrotoxicosis as pregnancy-associated thyrotoxicosis. A clinically significant number of women developed Graves' disease in the postpartum period in a single thyroid centre.
妊娠和分娩对甲状腺功能有显著影响。然而,妊娠期甲状腺毒症(GT)、妊娠期新发格雷夫斯病(妊娠期GD)、产后破坏性甲状腺毒症(PPT)和产后格雷夫斯甲状腺毒症(PPGD)的相对患病率尚未确定。
我们对2008年8月至2013年12月在熊本医院门诊就诊的4127例未经治疗的连续女性甲状腺毒症患者进行了前瞻性登记和回顾。4127名女性中有187名在妊娠期间或产后被新诊断为甲状腺毒症。我们调查了GT、妊娠期GD、PPT和PPGD新诊断的患病率,并比较了这些类型甲状腺毒症的特征。产后时期定义为分娩后十二个月。
在187名妊娠或产后妇女中,我们确定30例(16.0%)患有GT,13例(7.0%)患有妊娠期GD,42例(22.5%)患有PPT,102例(54.5%)患有PPGD。妊娠期间甲状腺毒症的发病时间,即GT和妊娠期GD,在妊娠10周时hCG达到峰值时延迟了几周。76%的PPT患者在分娩至产后4个月之间发生甲状腺毒症;另一方面,83.3%的PPGD患者在产后6个月或更晚发生甲状腺毒症。
我们将妊娠期甲状腺毒症、妊娠期新发格雷夫斯病、产后破坏性甲状腺毒症和产后格雷夫斯甲状腺毒症命名为妊娠相关甲状腺毒症。在一个单一的甲状腺中心,有相当数量的女性在产后时期患上了格雷夫斯病。