Faseru Babalola, Ellerbeck Edward F, Catley Delwyn, Gajewski Byron J, Scheuermann Taneisha S, Shireman Theresa I, Mussulman Laura M, Nazir Niaman, Bush Terry, Richter Kimber P
Department of Preventive Medicine and Public Health, University of Kansas Medical Center, 3901 Rainbow Boulevard, Kansas City, KS, 66160, USA.
University of Kansas Cancer Center, 3901 Rainbow Boulevard, Kansas City, KS, USA.
Trials. 2017 Aug 14;18(1):379. doi: 10.1186/s13063-017-2119-9.
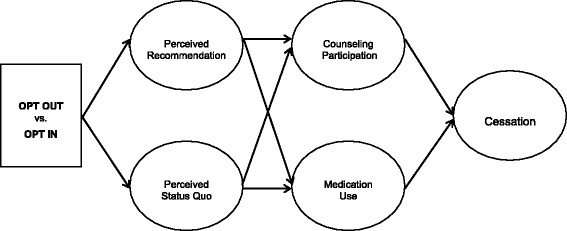
Most health care providers do not treat tobacco dependence routinely. This may in part be due to the treatment "default." Current treatment guidelines recommend that providers (1) ask patients if they are willing to quit and (2) provide cessation-focused medications and counseling only to smokers who state that they are willing to quit. The default is that patients have to "opt in" to receive cessation assistance: providers ask smokers if they are willing to quit, and only offer medications and cessation support to those who say "yes." This drastically limits the reach of cessation services because, at any given encounter, only one in three smokers say that they are ready to quit. The objective of this study is to determine the impact of providing all smokers with tobacco-cessation treatment unless they refuse it (OPT OUT) versus current practice-screening for readiness and only offering treatment to smokers who say they are ready to quit (OPT IN).
This individually randomized clinical trial is conducted in a tertiary-care hospital. We will conduct the trial among up to 1000 randomly selected hospitalized smokers to determine the population impact of changing the treatment default, identify mediators of outcome, and determine the cost-effectiveness of this new, highly proactive approach. This is a population-based study that targets an endpoint of vital interest; applies minimal eligibility criteria to broaden generalizability; and utilizes hospital staff for interventions to ensure long-term sustainability. The study employs delayed consent and an innovative Bayesian adaptive design to evaluate a major shift in our approach to care. If effective, this change would expand the reach of tobacco-cessation treatment from 30% to 100% of smokers.
Regardless of outcome, the trial will provide a model of how to alter and evaluate the impact of health care defaults. If OPT OUT proves to be more effective, it will expand the population eligible for cessation treatment by over 300%. It will also simplify the tobacco-cessation treatment algorithm, and relieve busy health care providers of the burden of evaluating readiness to quit.
Clinical Trials Registration, ID: NCT02721082 . Registered on 22 March 2016.
大多数医疗服务提供者并不常规治疗烟草依赖。这在一定程度上可能是由于治疗“默认方式”。当前的治疗指南建议医疗服务提供者:(1)询问患者是否愿意戒烟;(2)仅向表示愿意戒烟的吸烟者提供以戒烟为重点的药物和咨询服务。默认方式是患者必须“选择加入”才能获得戒烟帮助:医疗服务提供者询问吸烟者是否愿意戒烟,并且只向回答“愿意”的吸烟者提供药物和戒烟支持。这极大地限制了戒烟服务的覆盖范围,因为在任何一次就诊时,只有三分之一的吸烟者表示他们准备好戒烟。本研究的目的是确定为所有吸烟者提供戒烟治疗(除非他们拒绝,即“选择退出”)与当前做法(筛查戒烟意愿,仅向表示准备好戒烟的吸烟者提供治疗,即“选择加入”)相比的影响。
这项个体随机临床试验在一家三级护理医院进行。我们将在多达1000名随机选择的住院吸烟者中开展试验,以确定改变治疗默认方式对人群的影响,确定结果的调节因素,并确定这种全新的、高度积极主动的方法的成本效益。这是一项基于人群的研究,以一个至关重要的终点为目标;应用极少的纳入标准以扩大普遍性;并利用医院工作人员进行干预以确保长期可持续性。该研究采用延迟同意和创新的贝叶斯适应性设计来评估我们护理方法的重大转变。如果有效,这一改变将使戒烟治疗的覆盖范围从30%的吸烟者扩大到100%。
无论结果如何,该试验都将提供一个如何改变和评估医疗保健默认方式影响的模型。如果“选择退出”被证明更有效,它将使有资格接受戒烟治疗的人群扩大超过300%。它还将简化戒烟治疗方案,并减轻忙碌的医疗服务提供者评估戒烟意愿所带来的负担。
临床试验注册,编号:NCT02721082。于2016年3月22日注册。