Villois Paola, Grimaldi David, Spadaro Savino, Shinotsuka Claudia Righy, Fontana Vito, Scolletta Sabino, Franchi Federico, Vincent Jean-Louis, Creteur Jacques, Taccone Fabio Silvio
Department of Intensive Care, Erasme Hospital, Université Libre de Bruxelles (ULB), Route de Lennik, 808, 1070, Brussels, Belgium.
Department of Morphological Surgery and Experimental Medicine, Arcispedale Sant'Anna, Università di Ferrara, Via AldoMoro, 8, 44121, Ferrara, Italy.
Ann Intensive Care. 2017 Aug 14;7(1):85. doi: 10.1186/s13613-017-0308-z.
A decrease in circulating lymphocytes has been described as a marker of poor prognosis after septic shock; however, scarce data are available after cardiac arrest (CA). The aim of this study was to evaluate the impact of lymphopaenia after successful cardiopulmonary resuscitation.
This is a retrospective analysis of an institutional database including all adult CA patients admitted to the intensive care unit (ICU) between January 2007 and December 2014 who survived for at least 24 h. Demographic, CA-related data and ICU mortality were recorded as was lymphocyte count on admission and for the first 48 h. A cerebral performance category score of 3-5 at 3 months was considered as an unfavourable neurological outcome.
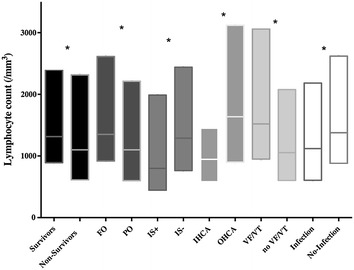
Data from 377 patients were analysed (median age: 62 [IQRs: 52-75] years). Median time to return of spontaneous circulation (ROSC) was 15 [8-25] min and 232 (62%) had a non-shockable initial rhythm. ICU mortality was 58% (n = 217) and 246 (65%) patients had an unfavourable outcome at 3 months. The median lymphocyte count on admission was 1208 [700-2350]/mm and 151 (40%) patients had lymphopaenia (lymphocyte count <1000/mm). Predictors of lymphopaenia on admission were older age, a shorter time to ROSC, prior use of corticosteroid therapy and high C-reactive protein levels on admission. ICU non-survivors had lower lymphocyte counts on admission than survivors (1100 [613-2317] vs. 1316 [891-2395]/mm; p = 0.05) as did patients with unfavourable compared to those with favourable neurological outcomes (1100 [600-2013] vs. 1350 [919-2614]/mm; p = 0.003). However, lymphopaenia on admission was not an independent predictor of poor outcomes in the entire population, but only among OHCA patients.
A low lymphocyte count is common in CA survivors and is associated with poor outcome after OHCA.
循环淋巴细胞减少被认为是感染性休克预后不良的一个指标;然而,关于心脏骤停(CA)后的数据却很少。本研究的目的是评估心肺复苏成功后淋巴细胞减少的影响。
这是一项对机构数据库的回顾性分析,纳入了2007年1月至2014年12月期间入住重症监护病房(ICU)且存活至少24小时的所有成年CA患者。记录了人口统计学、与CA相关的数据以及ICU死亡率,同时记录了入院时和最初48小时的淋巴细胞计数。3个月时脑功能分类评分为3 - 5分被视为不良神经学结局。
分析了377例患者的数据(中位年龄:62 [四分位间距:52 - 75]岁)。自主循环恢复(ROSC)的中位时间为15 [8 - 25]分钟,232例(62%)患者初始心律不可电击。ICU死亡率为58%(n = 217),246例(65%)患者在3个月时预后不良。入院时淋巴细胞计数中位数为1208 [700 - 2350]/mm³,151例(40%)患者存在淋巴细胞减少(淋巴细胞计数<1000/mm³)。入院时淋巴细胞减少的预测因素包括年龄较大、ROSC时间较短、既往使用皮质类固醇治疗以及入院时高C反应蛋白水平。ICU非幸存者入院时的淋巴细胞计数低于幸存者(1100 [613 - 2317] vs. 1316 [891 - 2395]/mm³;p = 0.05),神经学结局不良的患者低于结局良好的患者(1100 [600 - 2013] vs. 1350 [919 - 2614]/mm³;p = 0.003)。然而,入院时淋巴细胞减少并非整个人群不良结局的独立预测因素,仅在院外心脏骤停(OHCA)患者中是。
CA幸存者中淋巴细胞计数低很常见,且与OHCA后的不良结局相关。