Hungerford Daniel, Smith Katie, Tucker Angela, Iturriza-Gómara Miren, Vivancos Roberto, McLeonard Catherine, A Cunliffe Nigel, French Neil
Institute of Infection and Global Health, University of Liverpool, Liverpool, L69 7BE, UK.
Field Epidemiology Service, National Infection Service, Public Health England, Liverpool, L1 1JF, UK.
BMC Infect Dis. 2017 Aug 15;17(1):569. doi: 10.1186/s12879-017-2613-4.
Rotavirus was the leading cause of acute gastroenteritis (AGE) in infants and young children prior to the introduction of routine vaccination. Since 2006 there have been two licensed vaccines available; with successful clinical trials leading the World Health Organization to recommend rotavirus vaccination for all children worldwide. In order to inform immunisation policy we have conducted a systematic review and meta-analysis of observation studies to assess population effectiveness against acute gastroenteritis.
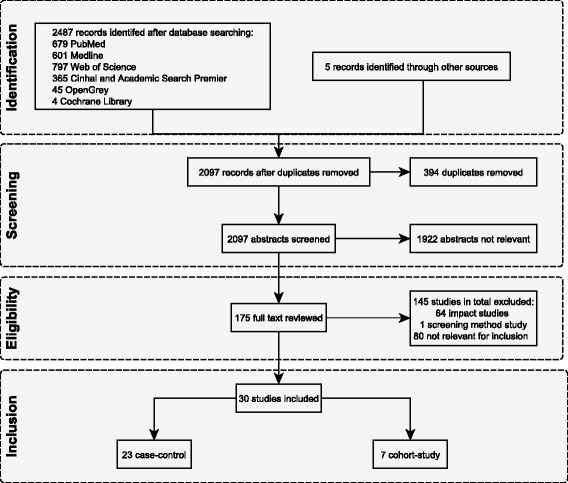
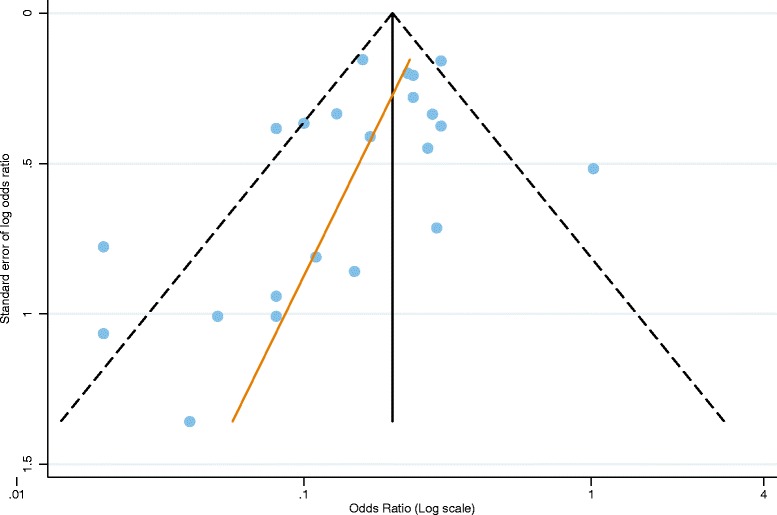
We systematically searched PubMed, Medline, Web of Science, Cinhal and Academic Search Premier and grey literature sources for studies published between January 2006 and April 2014. Studies were eligible for inclusion if they were observational measuring population effectiveness of rotavirus vaccination against health care attendances for rotavirus gastroenteritis or AGE. To evaluate study quality we use used the Newcastle-Ottawa Scale for non-randomised studies, categorising studies by risk of bias. Publication bias was assessed using funnel plots. If two or more studies reported a measure of vaccine effectiveness (VE), we conducted a random effects meta-analysis. We stratified analyses by World Bank country income level and used study quality in sensitivity analyses.
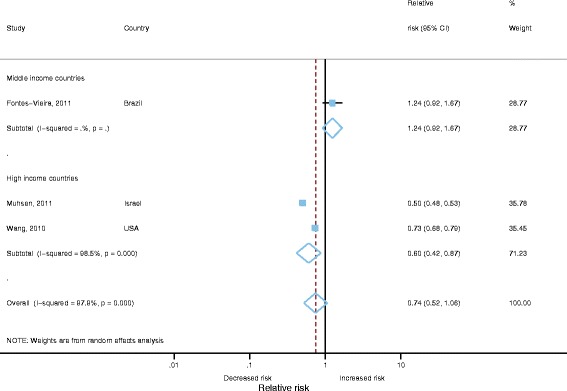
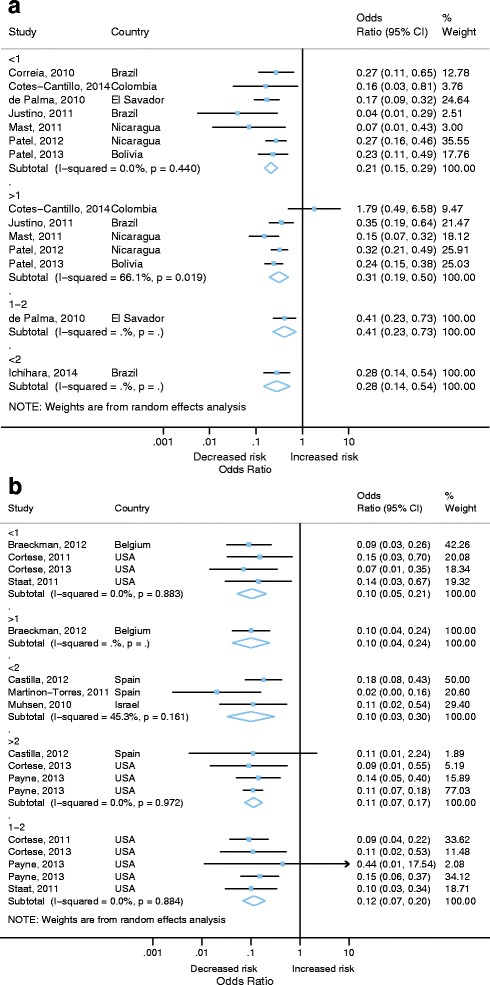
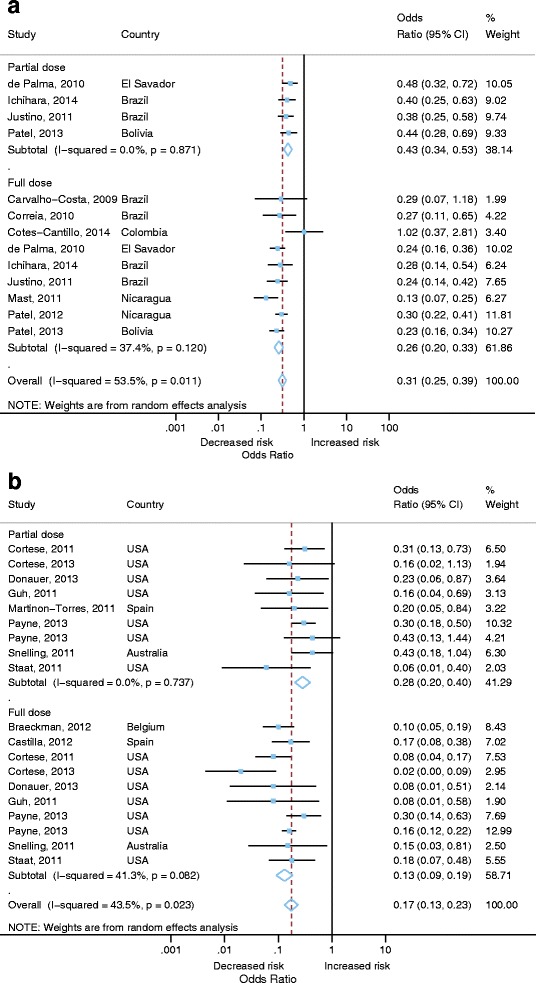
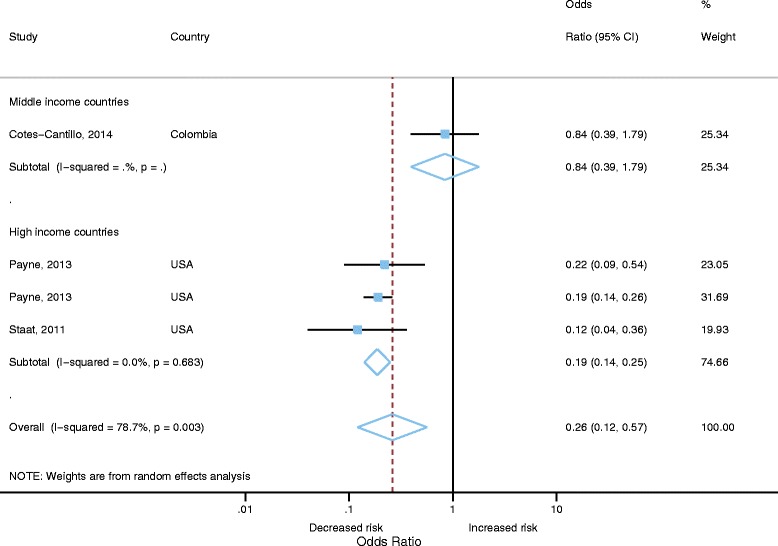
We identified 30 studies, 19 were from high-income countries and 11 from middle-income countries. Vaccine effectiveness against hospitalization for laboratory confirmed rotavirus gastroenteritis was highest in high-income countries (89% VE; 95% CI 84-92%) compared to middle-income countries (74% VE; 95% CI 67-80%). Vaccine effectiveness was higher for those receiving the complete vaccine schedule (81% VE; 95% CI 75-86%) compared to partial schedule (62% VE; 95% CI 55-69%). Two studies from high-income countries measured VE against community consultations for AGE with a pooled estimate of 40% (95% CI 13-58%; 2 studies).
We found strong evidence to further support the continued use of rotavirus vaccines. Vaccine effectiveness was similar to that reported in clinical trials for both high and middle-income countries. There is limited data from Low income settings at present. There was lower effectiveness against milder disease. Further studies, should continue to report effectiveness against AGE and less-severe rotavirus disease because as evidenced by pre-vaccine introduction studies this is likely to contribute the greatest burden on healthcare resources, particularly in high-income countries.
在常规疫苗接种引入之前,轮状病毒是婴幼儿急性胃肠炎(AGE)的主要病因。自2006年以来,已有两种获得许可的疫苗;成功的临床试验促使世界卫生组织建议全球所有儿童接种轮状病毒疫苗。为了为免疫政策提供依据,我们对观察性研究进行了系统评价和荟萃分析,以评估针对急性胃肠炎的人群有效性。
我们系统检索了PubMed、Medline、Web of Science、Cinhal和Academic Search Premier以及灰色文献来源,查找2006年1月至2014年4月期间发表的研究。如果研究是观察性的,测量轮状病毒疫苗针对因轮状病毒胃肠炎或AGE而就医的人群有效性,则符合纳入条件。为了评估研究质量,我们使用纽卡斯尔-渥太华量表对非随机研究进行评估,根据偏倚风险对研究进行分类。使用漏斗图评估发表偏倚。如果两项或更多研究报告了疫苗有效性(VE)的测量值,我们进行随机效应荟萃分析。我们按世界银行国家收入水平分层分析,并在敏感性分析中使用研究质量。
我们确定了30项研究,其中19项来自高收入国家,11项来自中等收入国家。与中等收入国家(疫苗有效性74%;95%可信区间67 - 80%)相比,高收入国家针对实验室确诊的轮状病毒胃肠炎住院的疫苗有效性最高(疫苗有效性89%;95%可信区间84 - 92%)。与部分接种程序(疫苗有效性62%;95%可信区间55 - 69%)相比,接受完整疫苗接种程序的人群疫苗有效性更高(疫苗有效性81%;95%可信区间75 - 86%)。来自高收入国家的两项研究测量了针对因AGE进行社区咨询的疫苗有效性,合并估计值为40%(95%可信区间13 - 58%;2项研究)。
我们发现有力证据进一步支持继续使用轮状病毒疫苗。高收入和中等收入国家的疫苗有效性与临床试验报告的相似。目前低收入地区的数据有限。针对较轻疾病的有效性较低。应继续开展进一步研究,报告针对AGE和不太严重的轮状病毒疾病的有效性,因为疫苗接种前的研究表明,这可能给医疗资源带来最大负担,尤其是在高收入国家。