Frühauf Filip, Zikan Michal, Semeradova Ivana, Dundr Pavel, Nemejcova Kristyna, Dusek Ladislav, Cibula David, Fischerova Daniela
Gynecologic Oncology Centre, Department of Obstetrics and Gynecology, First Faculty of Medicine, Charles University, General University Hospital, Prague, Czech Republic.
Department of Pathology, First Faculty of Medicine, Charles University, General University Hospital, Prague, Czech Republic.
Biomed Res Int. 2017;2017:1318203. doi: 10.1155/2017/1318203. Epub 2017 Jul 24.
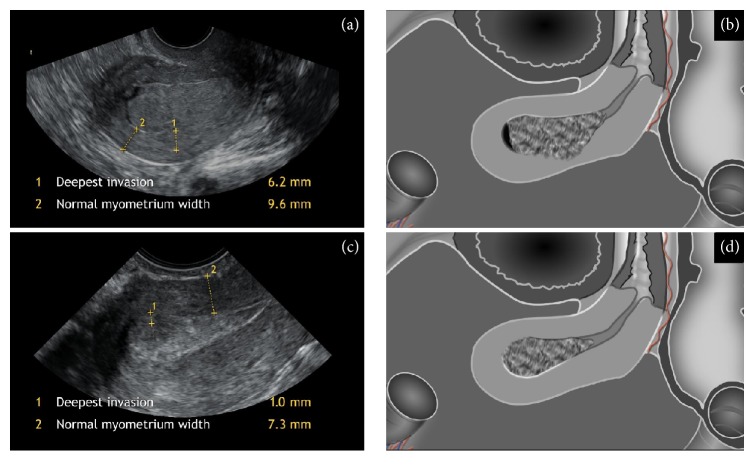
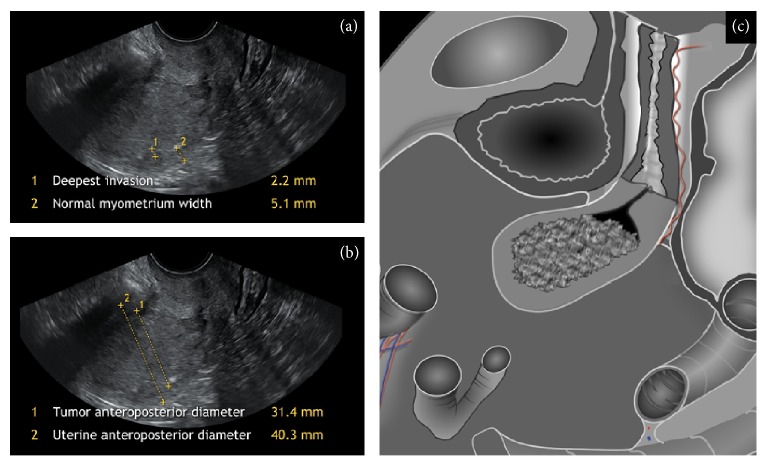
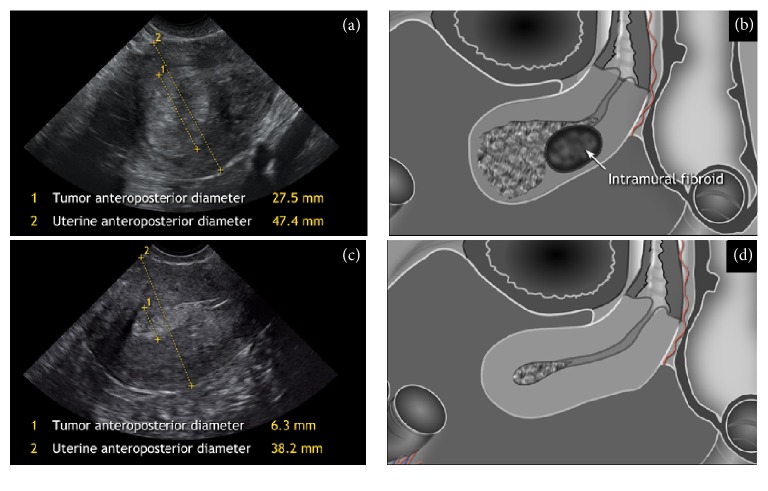
The aim of this study was to assess the diagnostic accuracy of subjective ultrasound evaluation of myometrial invasion of endometrial cancer and to compare its accuracy to objective methods. All consecutive patients with histologically proven endometrial cancer, who underwent ultrasound evaluation followed by surgical staging between January 2009 and December 2011, were prospectively enrolled. Myometrial invasion was evaluated by subjective assessment using ultrasound (<50% or ≥50%) and calculated as deepest invasion/normal myometrium ratio (Gordon's ratio) and as tumor/uterine anteroposterior diameter ratio (Karlsson's ratio). Histological assessment from hysterectomy was considered the gold standard. Altogether 210 patients were prospectively included. Subjective assessment and two objective ratios were found to be statistically significant predictors of the myometrial invasion (AUC = 0.65, value < 0.001). Subjective assessment was confirmed as the most reliable method to assess myometrial invasion (79.3% sensitivity, 73.2% specificity, and 75.7% overall accuracy). Deepest invasion/normal myometrium (Gordon's) ratio (cut-off 0.5) reached 69.6% sensitivity, 65.9% specificity, and 67.3% overall accuracy. Tumor/uterine anteroposterior diameter (Karlsson's) ratio with the same cut-off reached 56.3% sensitivity, 76.4% specificity, and 68.1% overall accuracy. The subjective ultrasound evaluation of myometrial invasion performed better than objective methods in nearly all measures but showed statistically significantly better outcomes only in case of sensitivity.
本研究的目的是评估主观超声评估子宫内膜癌肌层浸润的诊断准确性,并将其准确性与客观方法进行比较。前瞻性纳入了2009年1月至2011年12月期间所有经组织学证实为子宫内膜癌且接受了超声评估并随后进行手术分期的连续患者。通过超声主观评估(<50%或≥50%)来评估肌层浸润,并计算为最深浸润/正常肌层比值(戈登比值)和肿瘤/子宫前后径比值(卡尔森比值)。子宫切除术后的组织学评估被视为金标准。总共前瞻性纳入了210例患者。主观评估和两个客观比值被发现是肌层浸润的统计学显著预测指标(AUC = 0.65,P值<0.001)。主观评估被确认为评估肌层浸润最可靠的方法(敏感性79.3%,特异性73.2%,总体准确性75.7%)。最深浸润/正常肌层(戈登)比值(临界值0.5)的敏感性为69.6%,特异性为65.9%,总体准确性为67.3%。相同临界值的肿瘤/子宫前后径(卡尔森)比值的敏感性为56.3%,特异性为76.4%,总体准确性为68.1%。主观超声评估肌层浸润在几乎所有指标上都比客观方法表现更好,但仅在敏感性方面显示出统计学上显著更好的结果。