Thongprayoon Charat, Cheungpasitporn Wisit, Srivali Narat, Kittanamongkolchai Wonngarm, Sakhuja Ankit, Greason Kevin L, Kashani Kianoush B
Division of Nephrology and Hypertension, Mayo Clinic, Rochester, Minnesota, United States of America.
Division of Pulmonary and Critical Care Medicine, Mayo Clinic, Rochester, Minnesota, United States of America.
PLoS One. 2017 Aug 17;12(8):e0183350. doi: 10.1371/journal.pone.0183350. eCollection 2017.
This study aimed to examine the association between renal recovery status at hospital discharge after acute kidney injury (AKI) and long-term mortality following transcatheter aortic valve replacement (TAVR).
We screened all adult patients who survived to hospital discharge after TAVR for aortic stenosis at a quaternary referral medical center from January 1, 2008, through June 30, 2014. An AKI was defined as an increase in serum creatinine level of 0.3 mg/dL or a relative increase of 50% from baseline. Renal outcome at the time of discharge was evaluated by comparing the discharge serum creatinine level to the baseline level. Complete renal recovery was defined as no AKI at discharge, whereas partial renal recovery was defined as AKI without a need for renal replacement therapy at discharge. No renal recovery was defined as a need for renal replacement therapy at discharge.
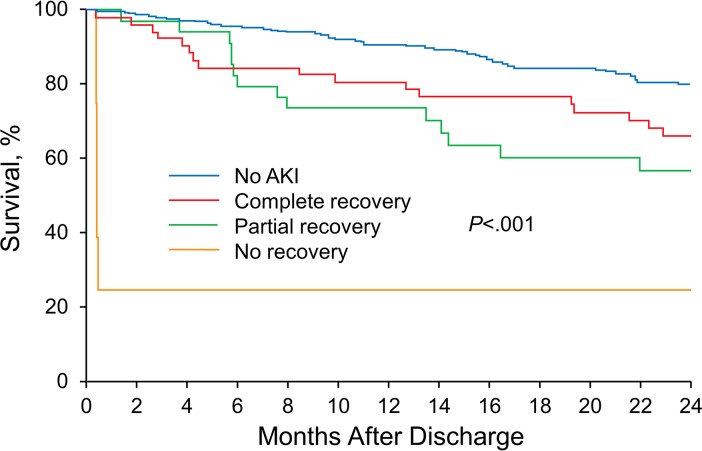
The study included 374 patients. Ninty-eight (26%) patients developed AKI during hospitalization: 55 (56%) had complete recovery; 39 (40%), partial recovery; and 4 (4%), no recovery. AKI development was significantly associated with increased risk of 2-year mortality (hazard ratio [HR], 2.20 [95% CI, 1.37-3.49]). For patients with AKI, the 2-year mortality rate for complete recovery was 34%; for partial recovery, 43%; and for no recovery, 75%; compared with 20% for patients without AKI (P < .001). In adjusted analysis, complete recovery (HR, 1.87 [95% CI, 1.03-3.23]); partial recovery (HR, 2.65 [95% CI, 1.40-4.71]) and no recovery (HR, 10.95 [95% CI, 2.59-31.49]) after AKI vs no AKI were significantly associated with increased risk of 2-year mortality.
The mortality rate increased for all patients with AKI undergoing TAVR. A reverse correlation existed for progressively higher risk of death and the extent of AKI recovery.
本研究旨在探讨急性肾损伤(AKI)后出院时的肾脏恢复状况与经导管主动脉瓣置换术(TAVR)后长期死亡率之间的关联。
我们筛选了2008年1月1日至2014年6月30日在一家四级转诊医疗中心因主动脉瓣狭窄接受TAVR后存活至出院的所有成年患者。AKI定义为血清肌酐水平升高0.3mg/dL或较基线水平相对升高50%。通过比较出院时血清肌酐水平与基线水平来评估出院时的肾脏结局。完全肾脏恢复定义为出院时无AKI,而部分肾脏恢复定义为出院时存在AKI但无需肾脏替代治疗。无肾脏恢复定义为出院时需要肾脏替代治疗。
该研究纳入了374例患者。98例(26%)患者在住院期间发生AKI:55例(56%)完全恢复;39例(40%)部分恢复;4例(4%)未恢复。发生AKI与2年死亡率风险增加显著相关(风险比[HR],2.20[95%CI,1.37 - 3.49])。对于发生AKI的患者,完全恢复的2年死亡率为34%;部分恢复的为43%;未恢复的为75%;而未发生AKI的患者为20%(P <.001)。在多因素分析中,AKI后完全恢复(HR,1.87[95%CI,1.03 - 3.23])、部分恢复(HR,2.65[95%CI,1.40 - 4.71])和未恢复(HR,10.95[95%CI,2.59 - 31.49])与未发生AKI相比,均与2年死亡率风险增加显著相关。
所有接受TAVR的AKI患者死亡率均升高。死亡风险逐渐升高与AKI恢复程度呈负相关。