Boddu Prajwal, Schlette Ellen, Thakral Beenu, Tang Guillin, Pemmaraju Naveen, Kadia Tapan, Ferrajoli Alessandra, Ravandi Farhad, Wierda William, Jain Nitin
Department of Leukemia, MD Anderson Cancer Center, The University of Texas, Houston, TX, USA.
Department of Hematopathology, MD Anderson Cancer Center, The University of Texas, Houston, TX, USA.
Hematol Oncol Stem Cell Ther. 2019 Sep;12(3):161-165. doi: 10.1016/j.hemonc.2017.07.004. Epub 2017 Aug 16.
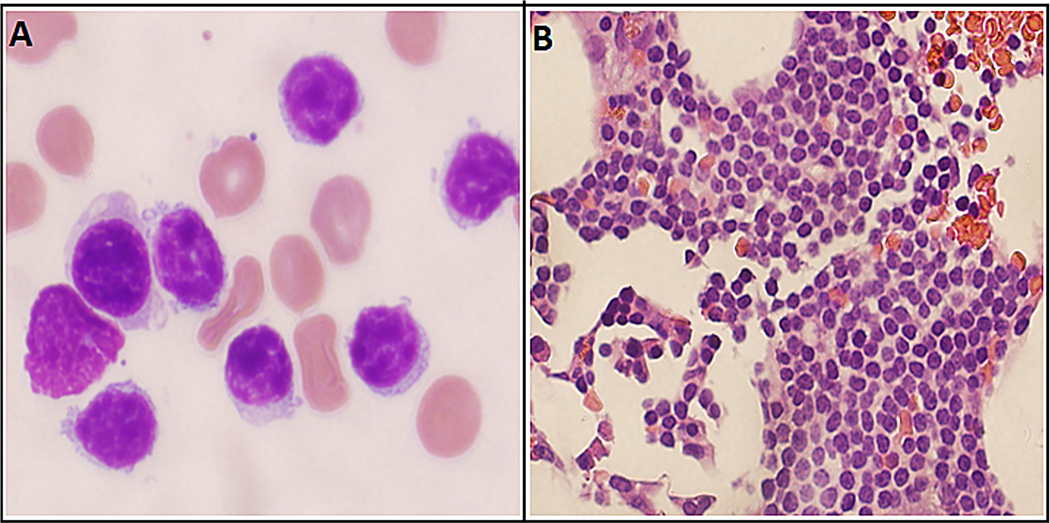
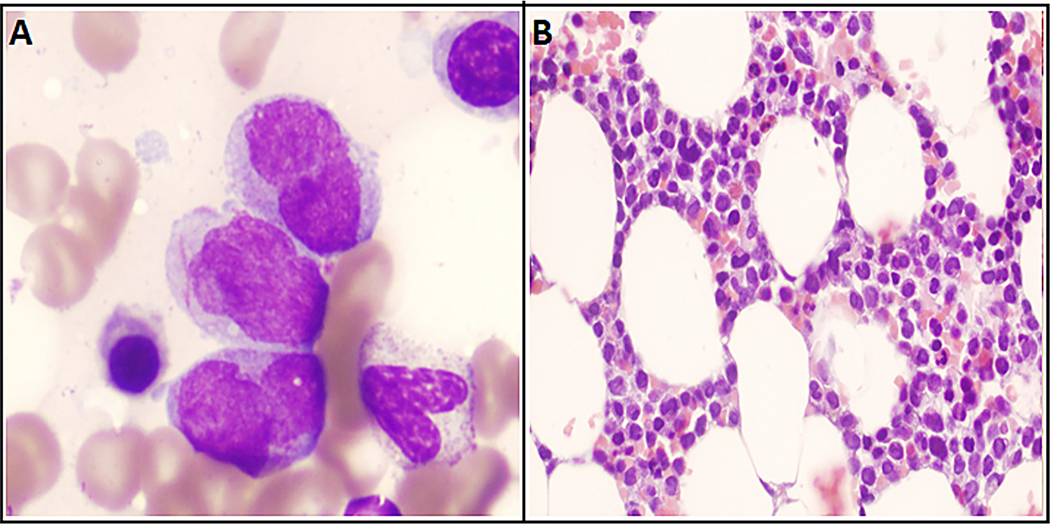
Chronic lymphocytic leukemia (CLL) is known to be associated rarely with myeloid malignancies such as acute myelogenous leukemia. In this article, we report an extremely rare occurrence of acute promyelocytic leukemia in a patient with CLL. A 71-year-old man first presented to our clinic with a diagnosis of CLL and worsening motor neuropathy symptoms. It was suspected that his CLL might be contributing to the neuropathy as a paraneoplastic syndrome, and he was treated with rituximab monotherapy in weekly doses for the 1st month and monthly treatments thereafter. By the end of his sixth monthly course of rituximab, the patient noted significant improvement in neuropathy symptoms but reported experiencing a new-onset worsening fatigue. He had new-onset cytopenias (white blood cells 1.6k/µL, hemoglobin 11.7g/dL, and platelet count 77k/µL). A bone marrow examination was performed; it showed a high percentage of progranulocytes (21%), which stained positive for myeloperoxidase (MPO) and demonstrated a fine granular pattern on the promyelocytic leukemia (PML) oncogenic domain immunofluorescence test. The diagnosis of acute promyelocytic leukemia was confirmed by fluorescence in situ hybridization, which showed a PML/RARα rearrangement in 46% of interphases. Flow cytometry was consistent with immunophenotype of acute promyelocytic leukemia and minimal residual CLL (0.07%). The patient was started promptly on all-trans-retinoic acid and arsenic trioxide induction regimen. Molecular remission was achieved after the first consolidation cycle. The patient is currently past his fourth consolidation cycle of all-trans-retinoic acid/arsenic trioxide and continues to be in complete remission. Our case illustrates that it is important for the physicians to be aware of coexistent hematologic and solid tumor malignancies in CLL, and maintain a low threshold for diagnostic testing based on grounds of low clinical suspicion.
已知慢性淋巴细胞白血病(CLL)很少与髓系恶性肿瘤如急性髓系白血病相关。在本文中,我们报告了1例CLL患者发生极罕见的急性早幼粒细胞白血病的情况。一名71岁男性首次到我们诊所就诊时被诊断为CLL,且运动神经病变症状加重。怀疑其CLL可能作为副肿瘤综合征导致神经病变,第1个月他接受每周一次的利妥昔单抗单药治疗,此后每月治疗一次。在他接受利妥昔单抗第6个疗程结束时,患者的神经病变症状有显著改善,但报告出现新发的疲劳加重。他出现了新发血细胞减少(白细胞1.6k/µL、血红蛋白11.7g/dL、血小板计数77k/µL)。进行了骨髓检查;结果显示早幼粒细胞比例较高(21%),髓过氧化物酶(MPO)染色呈阳性,在早幼粒细胞白血病(PML)致癌结构域免疫荧光试验中显示出细颗粒模式。荧光原位杂交证实了急性早幼粒细胞白血病的诊断,该检查显示46%的间期细胞存在PML/RARα重排。流式细胞术结果与急性早幼粒细胞白血病的免疫表型及微小残留CLL(0.07%)一致。患者立即开始接受全反式维甲酸和三氧化二砷诱导方案治疗。在第一个巩固周期后实现了分子缓解。该患者目前已完成全反式维甲酸/三氧化二砷的第4个巩固周期,仍处于完全缓解状态。我们的病例表明,医生了解CLL中共存的血液系统和实体肿瘤恶性肿瘤很重要,并基于低临床怀疑保持较低的诊断检查阈值。