Kamar Fareed B, Tam-Tham Helen, Thomas Chandra
Department of Medicine, Cumming School of Medicine, University of Calgary, Alberta, Canada.
Department of Community Health Sciences, Cumming School of Medicine, University of Calgary, Alberta, Canada.
Can J Kidney Health Dis. 2017 Jul 12;4:2054358117718538. doi: 10.1177/2054358117718538. eCollection 2017.
Conservative/palliative (nondialysis) management is an option for some individuals for treatment of stage 5 chronic kidney disease (CKD). Little is known about these individuals treated with conservative care in the Canadian setting.
To describe the characteristics of patients treated with conservative care for category G5 non-dialysis CKD in a Canadian context.
Retrospective chart review.
Urban nephrology center.
Patients with G5 non-dialysis CKD (estimated glomerular filtration rate <15 mL/min/1.73 m).
Baseline patient demographic and clinical characteristics of conservative care follow-up, advanced care planning, and death.
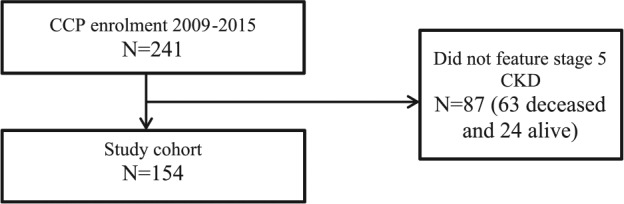
We undertook a descriptive analysis of individuals enrolled in a conservative care program between January 1, 2009, and June 30, 2015.
One hundred fifty-four patients were enrolled in the conservative care program. The mean age and standard deviation was 81.4 ± 9.0 years. The mean modified Charlson Comorbidity Index score was 3.4 ± 2.8. The median duration of conservative care participation was 11.5 months (interquartile range: 4-25). Six (3.9%) patients changed their modality to dialysis. One hundred three (66.9%) patients died during the study period. Within the deceased cohort, most (88.2%) patients completed at least some advanced care planning before death, and most (81.7%) of them died at their preferred place. Twenty-seven (26.7%) individuals died in hospital.
Single-center study with biases inherent to a retrospective study. Generalizability to non-Canadian settings may be limited.
We found that individuals who chose conservative care were very old and did not have high levels of comorbidity. Few individuals who chose conservative care changed modality and accepted dialysis. The proportions of engagement in advanced care planning and of death in place of choice were high in this population. Death in hospital was uncommon in this population.
保守/姑息(非透析)治疗是部分5期慢性肾脏病(CKD)患者的一种治疗选择。在加拿大,对于接受保守治疗的这些患者了解甚少。
描述加拿大背景下接受G5非透析CKD保守治疗患者的特征。
回顾性病历审查。
城市肾脏病中心。
G5非透析CKD患者(估计肾小球滤过率<15 mL/(min·1.73 m²))。
保守治疗随访的基线患者人口统计学和临床特征、临终关怀计划及死亡情况。
我们对2009年1月1日至2015年6月30日期间纳入保守治疗项目的患者进行了描述性分析。
154例患者纳入保守治疗项目。平均年龄及标准差为81.4±9.0岁。改良Charlson合并症指数平均评分为3.4±2.8。保守治疗参与的中位时长为11.5个月(四分位间距:4 - 25)。6例(3.9%)患者改变治疗方式接受透析。103例(66.9%)患者在研究期间死亡。在死亡队列中,大多数(88.2%)患者在死亡前至少完成了部分临终关怀计划,且大多数(81.7%)在其选择的地点死亡。27例(26.7%)患者在医院死亡。
单中心研究,存在回顾性研究固有的偏倚。对非加拿大环境的可推广性可能有限。
我们发现选择保守治疗的患者年龄很大且合并症程度不高。选择保守治疗的患者很少改变治疗方式并接受透析。该人群中参与临终关怀计划的比例及在选择地点死亡的比例很高。该人群在医院死亡并不常见。