Kumar Vasantha H S
Division of Neonatology, Department of Pediatrics, The Women & Children's Hospital of Buffalo, University at Buffalo, 219 Bryant Street, Buffalo, NY 14222-2006, USA.
Children (Basel). 2017 Aug 24;4(9):75. doi: 10.3390/children4090075.
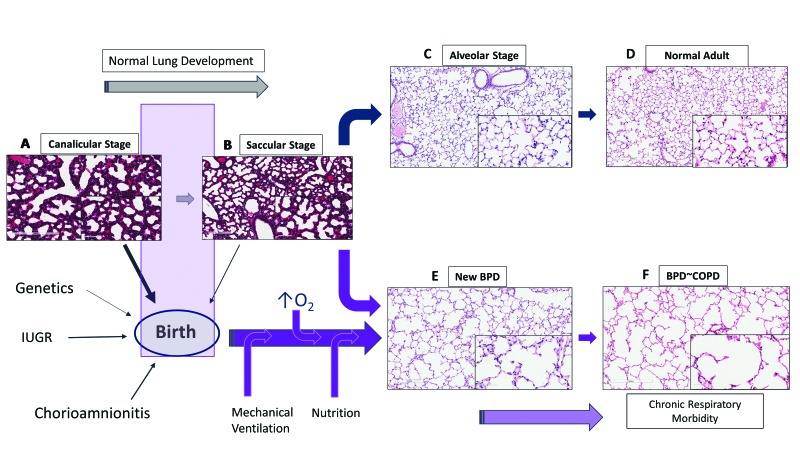
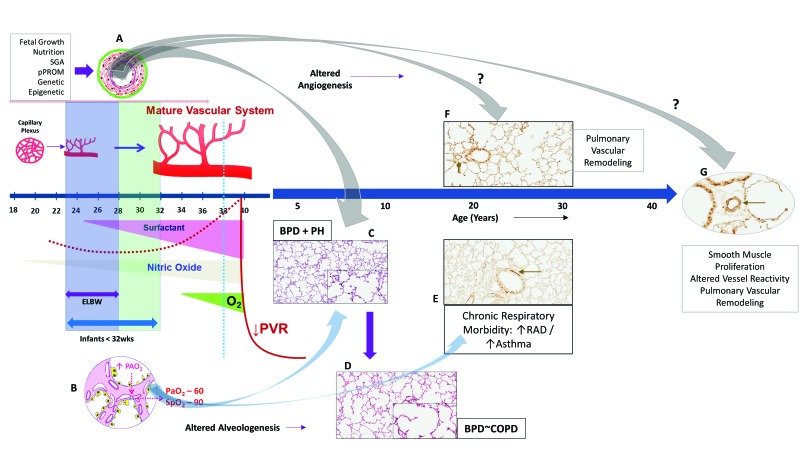
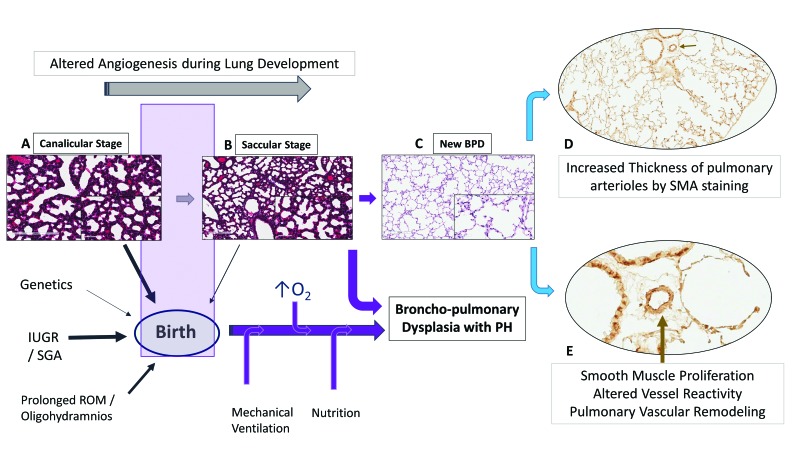
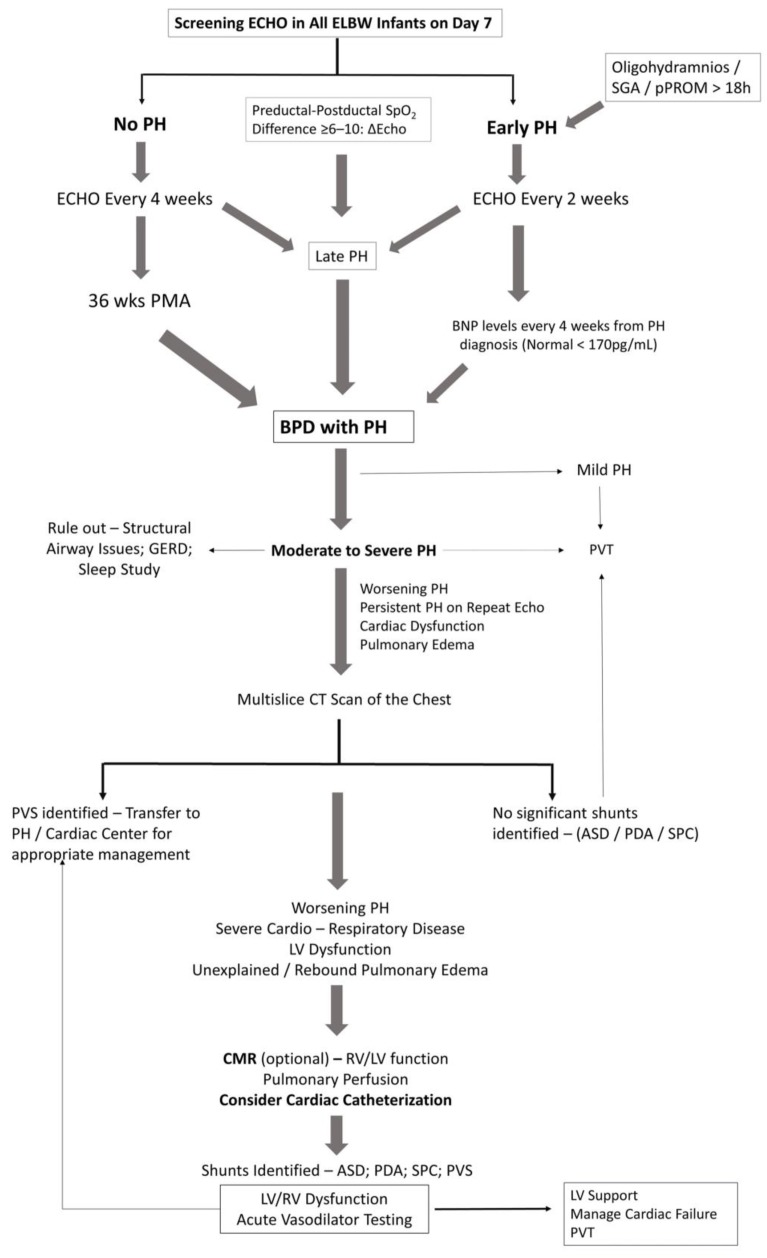
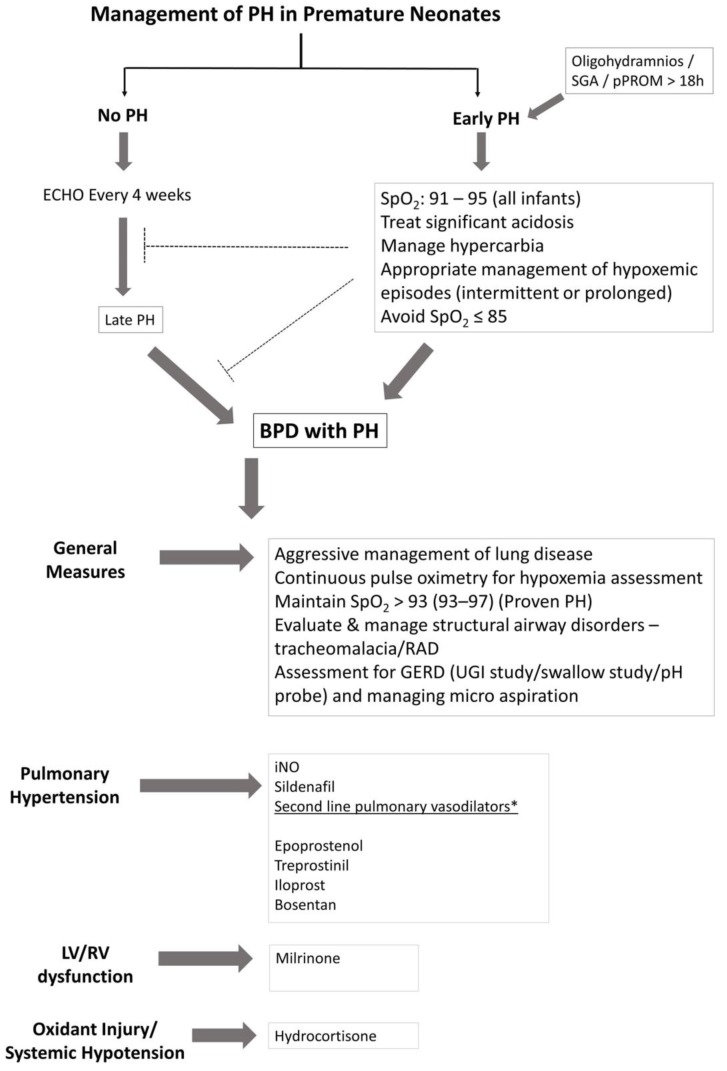
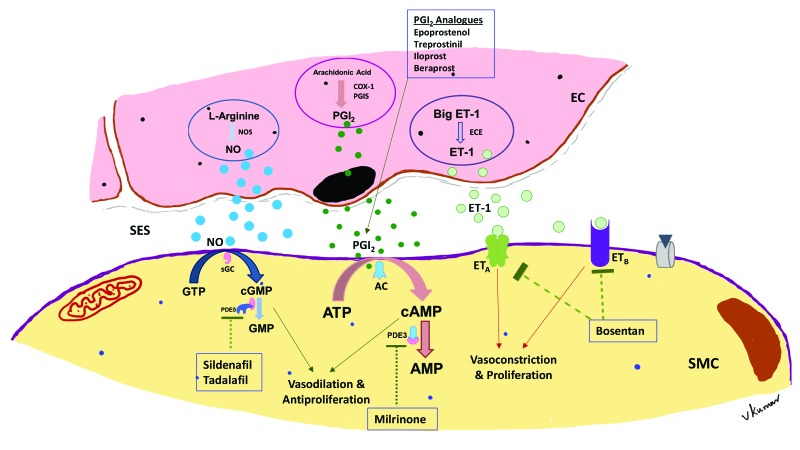
Bronchopulmonary dysplasia (BPD) is a form of chronic lung disease in premature infants following respiratory distress at birth. With increasing survival of extremely low birth weight infants, alveolar simplification is the defining lung characteristic of infants with BPD, and along with pulmonary hypertension, increasingly contributes to both respiratory morbidity and mortality in these infants. Growth restricted infants, infants born to mothers with oligohydramnios or following prolonged preterm rupture of membranes are at particular risk for early onset pulmonary hypertension. Altered vascular and alveolar growth particularly in canalicular and early saccular stages of lung development following mechanical ventilation and oxygen therapy, results in developmental lung arrest leading to BPD with pulmonary hypertension (PH). Early recognition of PH in infants with risk factors is important for optimal management of these infants. Screening tools for early diagnosis of PH are evolving; however, echocardiography is the mainstay for non-invasive diagnosis of PH in infants. Cardiac computed tomography (CT) and magnetic resonance are being used as imaging modalities, however their role in improving outcomes in these patients is uncertain. Follow-up of infants at risk for PH will help not only in early diagnosis, but also in appropriate management of these infants. Aggressive management of lung disease, avoidance of hypoxemic episodes, and optimal nutrition determine the progression of PH, as epigenetic factors may have significant effects, particularly in growth-restricted infants. Infants with diagnosis of PH are managed with pulmonary vasodilators and those resistant to therapy need to be worked up for the presence of cardio-vascular anomalies. The management of infants and toddlers with PH, especially following premature birth is an emerging field. Nonetheless, combination therapies in a multi-disciplinary setting improves outcomes for these infants.
支气管肺发育不良(BPD)是早产儿出生后呼吸窘迫所致的一种慢性肺部疾病。随着极低出生体重儿存活率的提高,肺泡简化是BPD患儿的典型肺部特征,并且与肺动脉高压一起,越来越多地导致这些患儿出现呼吸疾病和死亡。生长受限的婴儿、羊水过少母亲所生的婴儿或胎膜早破时间延长后出生的婴儿,尤其有早期发生肺动脉高压的风险。特别是在机械通气和氧疗后,肺发育的细支气管和早期囊泡阶段血管和肺泡生长改变,导致肺发育停滞,进而引发伴有肺动脉高压(PH)的BPD。对有危险因素的婴儿早期识别PH对于这些婴儿的最佳管理很重要。用于早期诊断PH的筛查工具正在不断发展;然而,超声心动图是婴儿PH无创诊断的主要手段。心脏计算机断层扫描(CT)和磁共振成像正在用作成像方式,然而它们在改善这些患者预后方面的作用尚不确定。对有PH风险的婴儿进行随访不仅有助于早期诊断,也有助于对这些婴儿进行适当管理。积极治疗肺部疾病、避免低氧血症发作以及优化营养决定了PH的进展,因为表观遗传因素可能有显著影响,特别是在生长受限的婴儿中。诊断为PH的婴儿采用肺血管扩张剂治疗,对治疗耐药的婴儿需要检查是否存在心血管异常。对患有PH的婴幼儿,尤其是早产之后的管理是一个新兴领域。尽管如此,多学科联合治疗可改善这些婴儿的预后。