Komo Toshiaki, Hihara Jun, Kanou Mikihiro, Kohashi Toshihiko, Ohmori Ichiro, Yoshimitsu Masanori, Ikeda Takuhiro, Nakashima Akira, Miguchi Masashi, Yamakita Ichiko, Mukaida Hidenori, Hirabayashi Naoki, Kaneko Mayumi
Department of Gastroenterological Surgery, Hiroshima City Asa Citizens Hospital, Japan.
Department of Gastroenterological Surgery, Hiroshima City Asa Citizens Hospital, Japan.
Int J Surg Case Rep. 2017;39:172-175. doi: 10.1016/j.ijscr.2017.08.005. Epub 2017 Aug 10.
Hamartomas are rare, benign tumors of the spleen. Few cases of splenic hamartomas associated with thrombocytopenia have been reported.
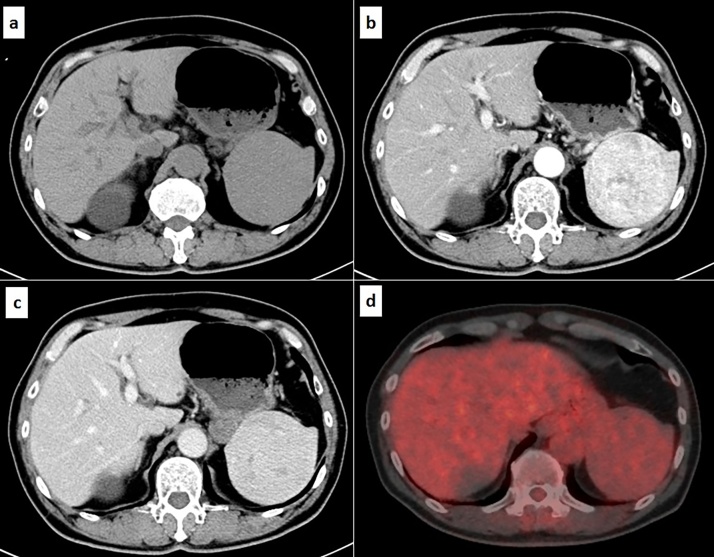
An asymptomatic 64-year-old man with myelodysplastic syndrome was found to have a splenic tumor. Laboratory tests were significant for thrombocytopenia, with a platelet count of 7.8×10/μL. Ultrasonography showed splenomegaly (10.8×6.6cm), and a hypoechoic splenic mass (8.0×7.0cm). Color doppler ultrasound revealed blood flow within the mass, and the mass density was homogeneous on abdominal computed tomography (CT). Contrast-enhanced CT showed heterogeneous enhancement of the splenic mass during the arterial phase. Positron emission tomography (PET)-CT showed no significant fludeoxyglucose (FDG) accumulation within the mass. The differential diagnosis included splenic hamartoma, splenic hemangioma, splenomegaly associated with extramedullary hematopoiesis, and malignant tumor, including solitary splenic metastasis. A laparoscopic splenectomy was performed due to the possibility of malignancy, the presence of thrombocytopenia, and the risk of splenic rupture. The resected specimen showed a localized, well-demarcated, 8.0×7.0cm splenic mass. Histological examination revealed abnormal red pulp proliferation and the absence of normal splenic structures. The patient's post-operative course was uneventful. His platelet count improved on post-operative day 1 and he was discharged on post-operative day 9. He remained in good health with a normal platelet count one month after surgery.
Making definitive preoperative diagnosis is difficult in splenic hamartomas. Surgery is necessary for diagnosis when malignancy cannot be ruled out.
Surgery may also improve symptoms of hypersplenism, including thrombocytopenia.
错构瘤是脾脏罕见的良性肿瘤。很少有脾错构瘤与血小板减少相关的病例报道。
一名64岁无症状的骨髓增生异常综合征男性被发现患有脾脏肿瘤。实验室检查显示血小板减少显著,血小板计数为7.8×10/μL。超声检查显示脾肿大(10.8×6.6cm),脾脏有一个低回声肿块(8.0×7.0cm)。彩色多普勒超声显示肿块内有血流,腹部计算机断层扫描(CT)显示肿块密度均匀。增强CT显示脾脏肿块在动脉期有不均匀强化。正电子发射断层扫描(PET)-CT显示肿块内无明显氟脱氧葡萄糖(FDG)积聚。鉴别诊断包括脾错构瘤、脾血管瘤、与髓外造血相关的脾肿大以及恶性肿瘤,包括孤立性脾转移瘤。由于存在恶性可能、血小板减少以及脾破裂风险,进行了腹腔镜脾切除术。切除标本显示一个局限性、边界清晰的8.0×7.0cm脾脏肿块。组织学检查显示红髓异常增生且无正常脾脏结构。患者术后恢复顺利。术后第1天血小板计数改善,术后第9天出院。术后1个月他身体健康,血小板计数正常。
脾错构瘤术前明确诊断困难。当不能排除恶性时,手术对于诊断是必要的。
手术也可能改善脾功能亢进症状,包括血小板减少。