Department of Obstetrics and Gynaecology, University of Nottingham, Royal Derby Hospital, Uttoxeter Road, Derby DE22 3DT, UK.
R&D Department, Derby Teaching Hospitals NHS Foundation Trust, Uttoxeter Road, Derby DE22 3NE, UK.
Hum Reprod. 2017 Aug 1;32(8):1631-1638. doi: 10.1093/humrep/dex227.
Would letrozole as a primary ovulation induction agent generate better pregnancy rates than clomiphene citrate (CC) in subfertile women with anovulatory polycystic ovarian syndrome (PCOS)?
Participants receiving letrozole as a primary treatment achieved a significantly (P = 0.022) higher clinical pregnancy rate per patient (61.2%) compared to CC (43.0%).
According to a recent Cochrane systematic review (2014), letrozole appears to improve live-birth (LB) and pregnancy rates in anovulatory women with PCOS, compared to CC. However, the review concluded that the quality of evidence was low due to poor reporting of study methods and possible publication bias.
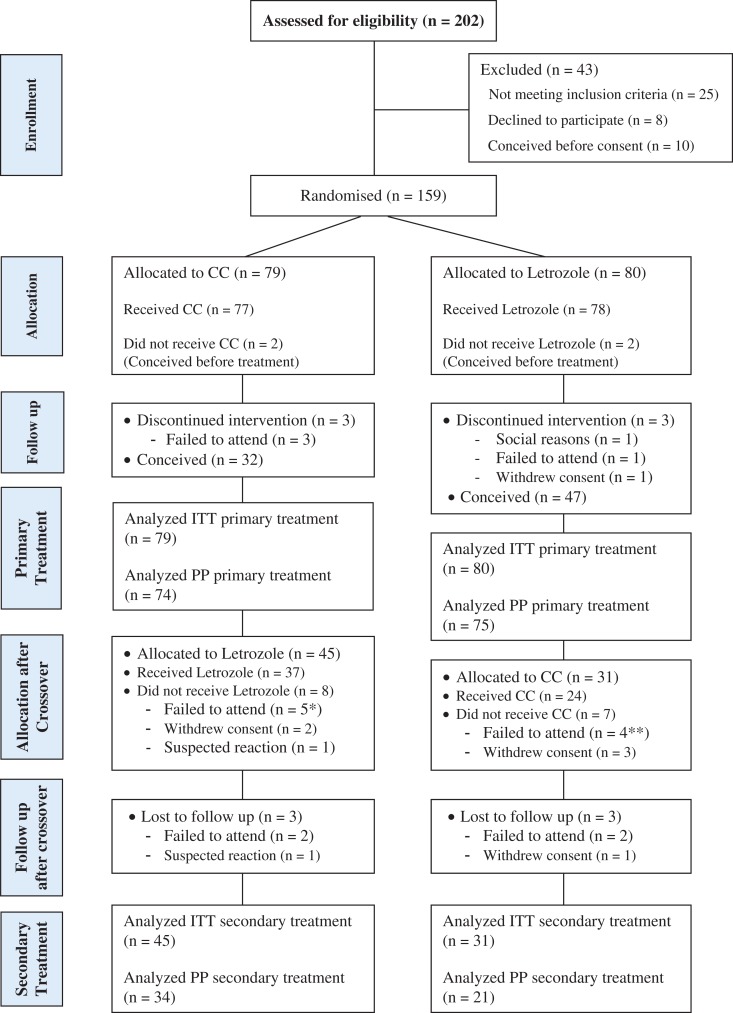
STUDY DESIGN, SIZE, DURATION: This double-blind randomized controlled trial (RCT) included 159 participants between April 2007 and June 2014. Subjects were randomly allocated to either CC (n = 79) or letrozole (n = 80) in a 1:1 ratio. Both drugs were encapsulated to look identical. Randomization was performed in mixed blocks and stratified by patients' BMI (<30 and 30-35 kg/m2).
PARTICIPANTS/MATERIALS, SETTING, METHODS: The trial included subfertile women diagnosed with PCOS. Treatment started with one tablet (CC 50 mg, letrozole 2.5 mg) increasing to two in non-responders and continuing until pregnancy or for up to six ovulatory cycles. Non-responders were crossed over to the other treatment after a 6-week break. Cycles were initially monitored with ultrasound follicle tracking then mid-luteal serum progesterone measurement in subsequent cycles.
Amongst the 159 participants included in the intention-to-treat analysis, four women conceived before treatment and six were lost-to-follow-up. The remaining 149 participants (74 on CC and 75 on letrozole) completed at least the first treatment. Women receiving letrozole achieved a significantly (P = 0.022; absolute difference [95% confidence interval] 18% [3-33%]) higher pregnancy rate (61.%) than those on CC (43%). The median number of treatment cycles received until pregnancy was significantly (log rank P = 0.038) smaller with letrozole (4[3-5] cycles) compared to CC (6[4-7] cycles). LB rates were not statistically (P = 0.089) different between the two groups, although there was a trend towards higher rates on letrozole (48.8%) compared to CC (35.4%). After the crossover, pregnancy and LB rates on letrozole (n = 45; 28.9 and 24.4%, respectively) were not statistically (P = 0.539 and P = 0.601) different from CC (n = 31; 22.6 and 19.4%).
LIMITATIONS, REASONS FOR CAUTION: One possible limitation of this trial may be the exclusion of PCOS women with BMI > 35 kg/m2, which would limit the applicability of the results in this subgroup of PCOS. However, this group of women are generally excluded from treatment in the majority of fertility centres, especially in Europe, due to the associated challenges and risks.
The results of this trial are consistent with the recent Cochrane systematic review. However, with its robust design, the current RCT provides more valid and compelling evidence for the superiority of letrozole over CC as a primary ovulation induction agent in PCOS women with 40% increase in pregnancy rates and with a shorter time-to-pregnancy. Furthermore, the participants in this RCT are a good representation of subfertile PCOS population receiving fertility treatment in Europe and worldwide. The results are therefore globally generalizable for clinical practice.
STUDY FUNDING/COMPETING INTEREST(S): This RCT was mainly funded by the R&D Funding Scheme of Derby Hospitals NHS Foundation Trust. The study also received funds from School of Medicine, University of Nottingham. The Trust R&D department was involved in the development of the protocol and the running of the trial. The trial was sponsored and monitored by the University of Nottingham. The authors have no conflicts of interest.
www.Clinicaltrials.gov: NCT00478504.
Registration was verified on 23/05/2007.
DATE OF FIRST PATIENT'S ENROLMENT: 25/04/2007.
来曲唑作为一线促排卵药物,在排卵障碍型多囊卵巢综合征(PCOS)的不孕妇女中,与枸橼酸氯米酚(CC)相比,是否能产生更好的妊娠率?
接受来曲唑作为主要治疗的参与者,每个患者的临床妊娠率(61.2%)明显(P=0.022)高于 CC(43.0%)。
根据最近的 Cochrane 系统评价(2014 年),与 CC 相比,来曲唑似乎能提高排卵障碍型 PCOS 妇女的活产(LB)和妊娠率。然而,该综述得出结论,由于研究方法的报告不佳和可能存在发表偏倚,证据质量较低。
研究设计、大小、持续时间:这是一项双盲随机对照试验(RCT),纳入了 2007 年 4 月至 2014 年 6 月期间的 159 名参与者。患者被随机分配至 CC(n=79)或来曲唑组(n=80),比例为 1:1。两种药物均封装为看起来相同的胶囊。随机分组采用混合分组,按患者 BMI(<30 和 30-35kg/m2)分层。
参与者/材料、地点、方法:该试验纳入了诊断为 PCOS 的不孕妇女。治疗开始时,给予每位患者一片(CC 50mg,来曲唑 2.5mg),无反应者增至两片,并持续治疗,直至妊娠或最多进行 6 个促排卵周期。无反应者在 6 周的休息期后交叉至另一种治疗。最初通过超声卵泡跟踪监测周期,然后在随后的周期中测量黄体中期血清孕激素水平。
在意向治疗分析中,159 名参与者中有 4 名在治疗前怀孕,6 名失访。其余 149 名参与者(CC 组 74 名,来曲唑组 75 名)至少完成了第一次治疗。接受来曲唑治疗的患者妊娠率(61.2%)明显(P=0.022;绝对差异[95%置信区间]18%[3-33%])高于 CC 组(43.0%)。来曲唑组接受治疗的妊娠周期中位数明显(对数秩检验 P=0.038)少于 CC 组(来曲唑组 4[3-5]个周期,CC 组 6[4-7]个周期)。两组的活产率虽无统计学差异(P=0.089),但来曲唑组(48.8%)略高于 CC 组(35.4%)。来曲唑组(n=45)和 CC 组(n=31)交叉后妊娠和活产率分别为 28.9%和 24.4%,均无统计学差异(P=0.539 和 P=0.601)。
局限性、谨慎的原因:本试验的一个可能局限性是排除了 BMI>35kg/m2 的 PCOS 妇女,这将限制本研究结果在这一亚组 PCOS 患者中的适用性。然而,由于相关的挑战和风险,这组妇女在大多数生育中心,特别是在欧洲,通常被排除在治疗之外。
本研究结果与最近的 Cochrane 系统评价一致。然而,由于其稳健的设计,本 RCT 为来曲唑作为 PCOS 妇女一线促排卵药物的优越性提供了更有力和更有说服力的证据,与 CC 相比,妊娠率提高了 40%,妊娠时间也缩短了。此外,本 RCT 的参与者很好地代表了在欧洲和全球范围内接受生育治疗的不孕 PCOS 人群。因此,研究结果具有普遍的临床实践意义。
研究资金/利益冲突:这项 RCT 主要由德比医院 NHS 基金会信托基金的研发资助计划资助。该研究还得到了诺丁汉大学医学院的资金支持。信托研发部门参与了方案的制定和试验的开展。该试验由诺丁汉大学赞助和监测。作者没有利益冲突。
www.Clinicaltrials.gov:NCT00478504。
2007 年 5 月 23 日验证。
2007 年 4 月 25 日。