Won Ki-Bum, Hur Seung-Ho, Nam Chang-Wook, Ann Soe Hee, Park Gyung-Min, Lee Sang-Gon, Kim Hyo-Eun, Cho Yun-Kyeong, Yoon Hyuck-Jun, Park Hyoung-Seob, Kim Hyungseop, Han Seongwook, Jeong Myung-Ho, Ahn Young-Keun, Rha Seung-Woon, Kim Chong-Jin, Cho Myeong-Chan, Kim Hyo-Soo, Chae Shung-Chull, Kim Kee-Sik, Kim Young-Jo, Kim Kwon-Bae, Barter Philip
Department of Internal Medicine, Ulsan University Hospital, University of Ulsan College of Medicine, Ulsan Department of Internal Medicine, Keimyung University Dongsan Medical Center, Daegu Department of Internal Medicine, Chonnam National University Hospital, Gwangju Department of Internal Medicine, Korea University Guro Hospital, Seoul Department of Internal Medicine, Kyunghee University Hospital, Seoul Department of Internal Medicine, Chungbuk National University Hospital, Cheongju Department of Internal Medicine, Seoul National University Hospital, Seoul Department of Internal Medicine, Kyungpook National University Hospital, Daegu Department of Internal Medicine, Daegu Catholic University Hospital, Daegu Department of Internal Medicine, Yeungnam University Hospital, Daegu, Korea Department of Internal Medicine, University of New South Wales, Sydney, Australia.
Medicine (Baltimore). 2017 Sep;96(35):e7180. doi: 10.1097/MD.0000000000007180.
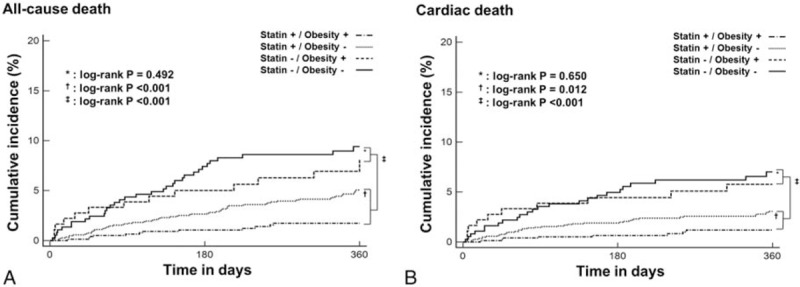
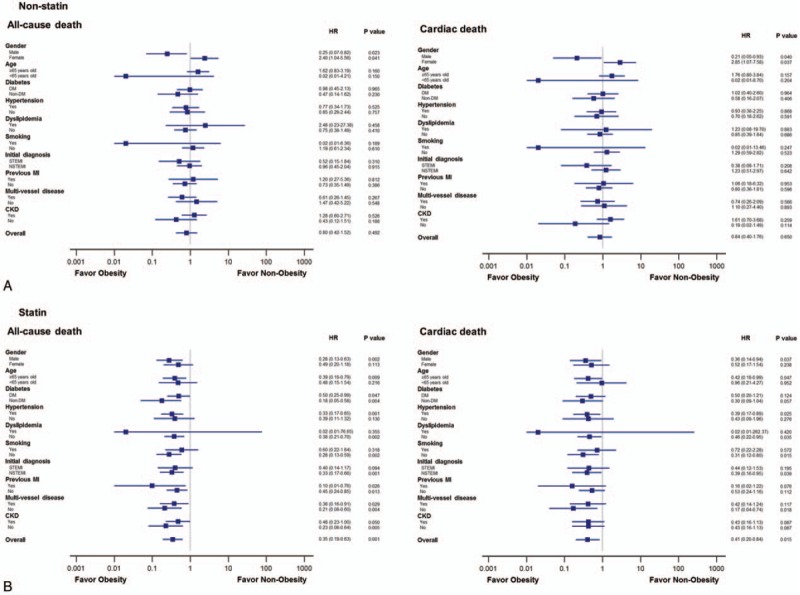
The phenomenon of obesity paradox after acute myocardial infarction (AMI) has been reported under strong recommendation of statin therapy. However, the impact of statin therapy on this paradox has not been investigated. This study investigated the impact of statin therapy on 1-year mortality according to obesity after AMI. A total of 2745 AMI patients were included from the Korea Acute Myocardial Infarction Registry after 1:4 propensity score matching analysis (n = 549 for nonstatin group and n = 2196 for statin group). Primary and secondary outcomes were all-cause and cardiac death, respectively. During 1-year follow-up, the incidence of all-cause (8.4% vs 3.7%) and cardiac (6.2% vs 2.3%) death was higher in nonstatin group than in statin (P < .001, respectively). In nonstatin group, the incidence of all-cause (7.2% vs 9.0%) and cardiac (5.5% vs 6.5%) death did not differ significantly between obese and nonobese patients. However, in statin group, obese patients had lower 1-year rate of all-cause (1.7% vs 4.8%) and cardiac (1.2% vs 2.9%) death (P < .05, respectively), and lower cumulative rates by Kaplan-Meier analysis of all-cause and cardiac death compared with nonobese patients (log-rank P < .05, respectively). The overall risk of all-cause death was significantly lower in obese than in nonobese patients only in statin group (hazard ratio: 0.35; P = .001). After adjusting for confounding factors, obesity was independently associated with decreased risk of all-cause death in statin group. In conclusion, the greater benefit of statin therapy for survival in obese patients is further confirmation of the obesity paradox after AMI.
在他汀类药物治疗的强烈推荐下,急性心肌梗死(AMI)后出现肥胖悖论的现象已被报道。然而,他汀类药物治疗对这一悖论的影响尚未得到研究。本研究调查了他汀类药物治疗对AMI后肥胖患者1年死亡率的影响。经过1:4倾向评分匹配分析后,从韩国急性心肌梗死登记处纳入了2745例AMI患者(非他汀组n = 549,他汀组n = 2196)。主要和次要结局分别是全因死亡和心源性死亡。在1年随访期间,非他汀组的全因死亡(8.4%对3.7%)和心源性死亡(6.2%对2.3%)发生率高于他汀组(P均<0.001)。在非他汀组中,肥胖和非肥胖患者的全因死亡(7.2%对9.0%)和心源性死亡(5.5%对6.5%)发生率无显著差异。然而,在他汀组中,肥胖患者的全因死亡(1.7%对4.8%)和心源性死亡(1.2%对2.9%)1年发生率较低(P均<0.05),并且与非肥胖患者相比,通过Kaplan-Meier分析的全因和心源性死亡累积发生率较低(对数秩检验P均<0.05)。仅在他汀组中,肥胖患者的全因死亡总体风险显著低于非肥胖患者(风险比:0.35;P = 0.001)。在调整混杂因素后,肥胖与他汀组全因死亡风险降低独立相关。总之,他汀类药物治疗对肥胖患者生存的更大益处进一步证实了AMI后的肥胖悖论。