Zhou Lei, Liu Weibin, Li Wei, Li Haifeng, Zhang Xu, Shang Huifang, Zhang Xu, Bu Bitao, Deng Hui, Fang Qi, Li Jimei, Zhang Hua, Song Zhi, Ou Changyi, Yan Chuanzhu, Liu Tao, Zhou Hongyu, Bao Jianhong, Lu Jiahong, Shi Huawei, Zhao Chongbo
Department of Neurology, Huashan Hospital, Fudan University, Shanghai, China.
Department of Neurology, The First Affiliated Hospital, Sun Yat-sen University, Guangzhou, China.
Ther Adv Neurol Disord. 2017 Sep;10(9):315-325. doi: 10.1177/1756285617721092. Epub 2017 Jul 26.
To determine the efficacy of low-dose, immediate-release tacrolimus in patients with myasthenia gravis (MG) with inadequate response to glucocorticoid therapy in a randomized, double-blind, placebo-controlled study.
Eligible patients had inadequate response to glucocorticoids (GCs) after ⩾6 weeks of treatment with prednisone ⩾0.75 mg/kg/day or 60-100 mg/day. Patients were randomized to receive 3 mg tacrolimus or placebo daily (orally) for 24 weeks. Concomitant glucocorticoids and pyridostigmine were allowed. Patients continued GC therapy from weeks 1-4; from week 5, the dose was decreased at the discretion of the investigator. The primary efficacy outcome measure was a reduction, relative to baseline, in quantitative myasthenia gravis (QMG) score assessed using a generalized linear model; supportive analyses used alternative models.
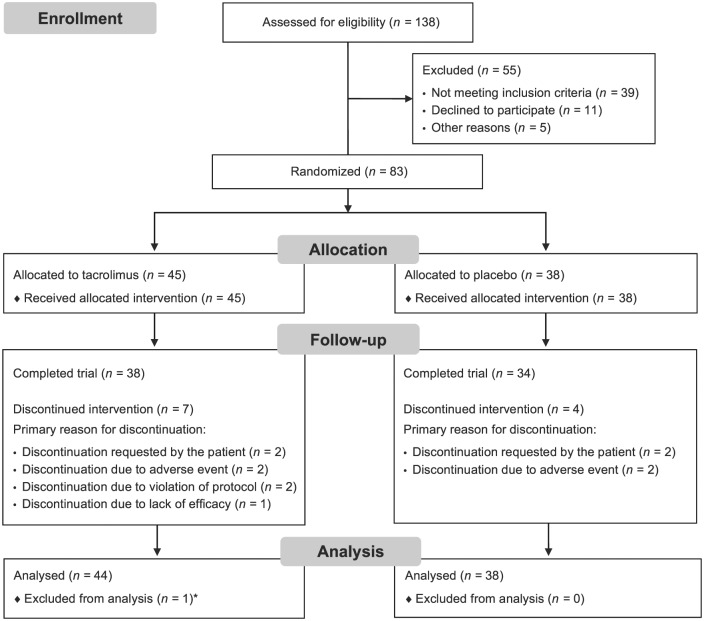
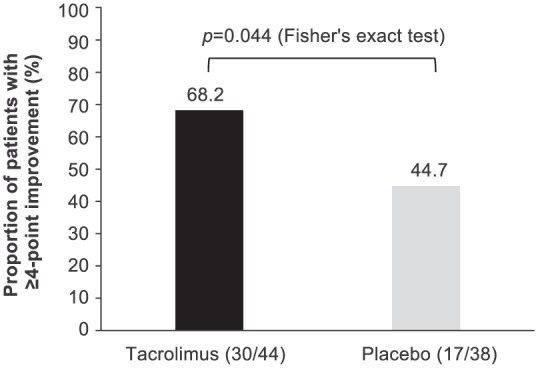
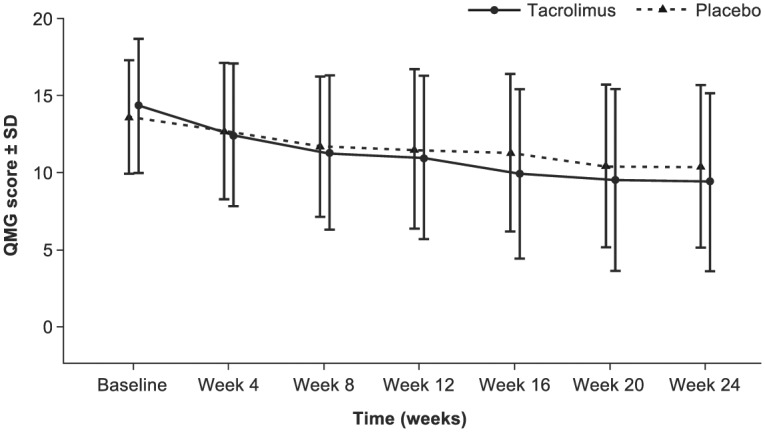
Of 138 patients screened, 83 [tacrolimus ( = 45); placebo ( = 38)] were enrolled and treated. The change in adjusted mean QMG score from baseline to week 24 was -4.9 for tacrolimus and -3.3 for placebo (least squares mean difference: -1.7, 95% confidence interval: -3.5, -0.1; = 0.067). A post-hoc analysis demonstrated a statistically significant difference for QMG score reduction of ⩾4 points in the tacrolimus group (68.2%) the placebo group (44.7%; = 0.044). Adverse event profiles were similar between treatment groups.
Tacrolimus 3 mg treatment for patients with MG and inadequate response to GCs did not demonstrate a statistically significant improvement in the primary endpoint placebo over 24 weeks; however, a post-hoc analysis demonstrated a statistically significant difference for QMG score reduction of ⩾4 points in the tacrolimus group the placebo group. This study was limited by the low number of patients, the absence of testing for acetylcholine receptor antibody and the absence of stratification by disease duration (which led to a disparity between the two groups). ClinicalTrials.gov identifier: NCT01325571.
在一项随机、双盲、安慰剂对照研究中,确定低剂量即释他克莫司对糖皮质激素治疗反应欠佳的重症肌无力(MG)患者的疗效。
符合条件的患者在接受泼尼松≥0.75 mg/kg/天或60 - 100 mg/天治疗≥6周后,对糖皮质激素(GCs)反应欠佳。患者被随机分为每日口服3 mg他克莫司或安慰剂,共24周。允许同时使用糖皮质激素和吡啶斯的明。患者在第1 - 4周继续GC治疗;从第5周起,剂量由研究者酌情减少。主要疗效指标是使用广义线性模型评估的重症肌无力定量(QMG)评分相对于基线的降低;支持性分析使用替代模型。
在138例筛查患者中,83例[他克莫司组(n = 45);安慰剂组(n = 38)]入组并接受治疗。从基线到第24周,他克莫司组调整后的平均QMG评分变化为 - 4.9分,安慰剂组为 - 3.3分(最小二乘均值差异: - 1.7,95%置信区间: - 3.5, - 0.1;P = 0.067)。事后分析显示,他克莫司组QMG评分降低≥4分的比例(68.2%)与安慰剂组(44.7%)相比有统计学显著差异(P = 0.044)。治疗组之间的不良事件情况相似。
对于MG且对GCs反应欠佳的患者,24周内3 mg他克莫司治疗在主要终点上相对于安慰剂未显示出统计学显著改善;然而,事后分析显示他克莫司组QMG评分降低≥4分与安慰剂组相比有统计学显著差异。本研究受患者数量少、未检测乙酰胆碱受体抗体以及未按病程分层(导致两组之间存在差异)的限制。ClinicalTrials.gov标识符:NCT01325571。