Department of Internal Medicine/Cardiology, University Heart Center Leipzig, Leipzig, Germany.
Klinik für Innere Medizin III, Kardiologie, Angiologie und Internistische Intensivmedizin, Saarland University Hospital, Homburg/Saar, Germany.
J Am Heart Assoc. 2017 Aug 10;6(8):e006196. doi: 10.1161/JAHA.117.006196.
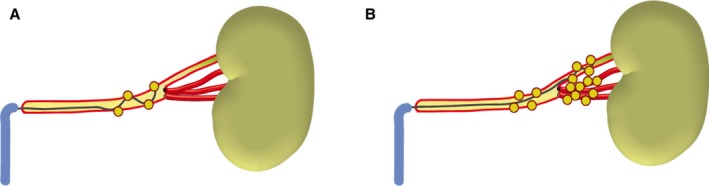
Single-electrode ablation of the main renal artery for renal sympathetic denervation showed mixed blood pressure (BP)-lowering effects. Further improvement of the technique seems crucial to optimize effectiveness of the procedure. Because sympathetic nerve fibers are closer to the lumen in the distal part of the renal artery, treatment of the distal main artery and its branches has been shown to reduce variability in treatment effects in preclinical studies and a recent randomized trial. Whether this optimized technique improves clinical outcomes remains uncertain. We report a 2-center experience of main renal artery and combined main renal artery plus branches renal denervation in patients with resistant hypertension using a multielectrode catheter.
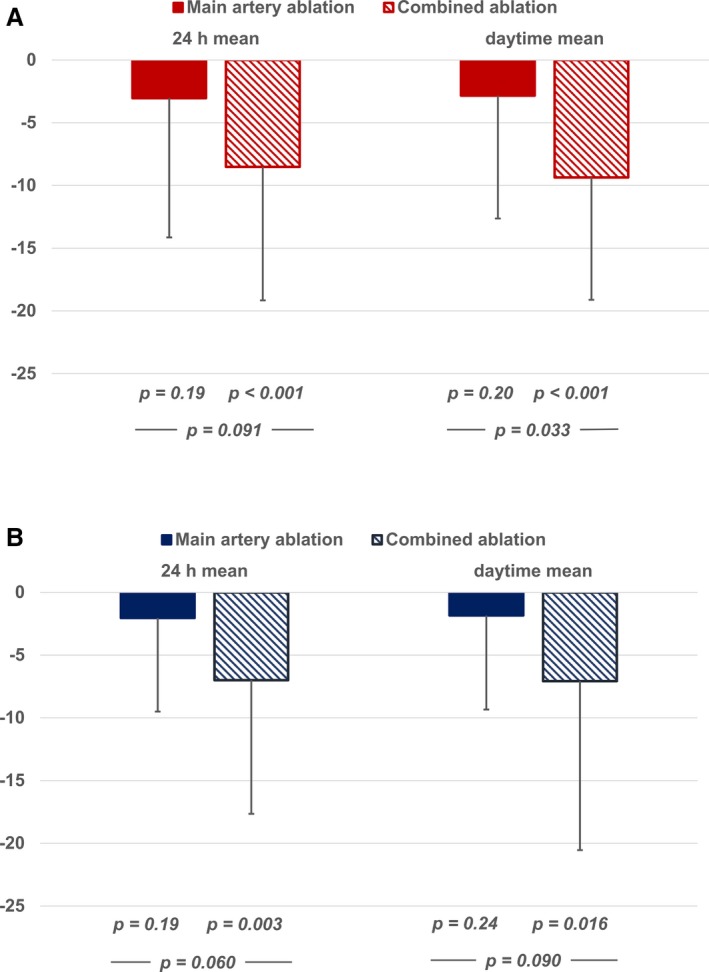
Twenty-five patients with therapy-resistant hypertension underwent renal sympathetic denervation with combined main renal artery and renal branch ablation and were compared to matched controls undergoing an ablation of the main renal artery only. BP change was assessed by ambulatory measurement at baseline and after 3 months. At baseline, BP was balanced between the groups. After 3 months, BP changed significantly in the combined ablation group (systolic/diastolic 24-hour mean and daytime mean BP -8.5±9.8/-7.0±10.7 and -9.4±9.8/-7.1±13.5 mm Hg, <0.001/0.003 and <0.001/0.016, respectively), but not in patients with main artery treatment (-3.5±11.1/-2.0±7.6 and -2.8±10.9/-1.8±7.7 mm Hg, =0.19/0.20 and 0.19/0.24, respectively). Systolic daytime BP was significantly more reduced in patients with combined ablation than in patients with main artery ablation (=0.033).
Combined ablation of the main renal artery and branches appears to improve BP-lowering efficacy and should be further investigated.
单电极消融主肾动脉进行肾交感神经去神经支配显示出混合的降压效果。进一步改进该技术似乎对于优化该程序的效果至关重要。由于交感神经纤维在肾动脉的远端更靠近管腔,因此在临床前研究和最近的一项随机试验中已经表明,治疗主肾动脉及其分支可以降低治疗效果的变异性。这种优化的技术是否能改善临床结果尚不确定。我们报告了 25 例采用多电极导管进行难治性高血压患者主肾动脉和联合主肾动脉加分支肾去神经支配的 2 中心经验。
25 例药物难治性高血压患者接受了联合主肾动脉和肾分支消融的肾交感神经去神经支配,并与仅接受主肾动脉消融的匹配对照组进行了比较。通过基线和 3 个月时的动态血压监测评估血压变化。基线时,两组的血压平衡。3 个月后,联合消融组的血压显著变化(24 小时平均收缩压/舒张压和日间平均收缩压/舒张压 -8.5±9.8/-7.0±10.7 和 -9.4±9.8/-7.1±13.5mmHg,<0.001/0.003 和 <0.001/0.016,分别),但主动脉治疗组的血压无变化(-3.5±11.1/-2.0±7.6 和 -2.8±10.9/-1.8±7.7mmHg,=0.19/0.20 和 0.19/0.24,分别)。联合消融组的日间收缩压显著降低(=0.033)。
联合消融主肾动脉和分支似乎可以提高降压效果,应进一步研究。