Department of Otorhinolaryngology, Head and Neck Surgery, University of Heidelberg, Im Neuenheimer Feld 400, 69120, Heidelberg, Germany.
Institute of Public Health, University of Heidelberg, INF 324, 69120, Heidelberg, Germany.
BMC Cancer. 2017 Sep 1;17(1):609. doi: 10.1186/s12885-017-3608-7.
Larynx preservation (LP) is recommended for up to low-volume T4 laryngeal cancer as an evidence-based treatment option that does not compromise survival. However, a reevaluation of the current literature raises questions regarding whether there is indeed reliable evidence to support larynx preservation for T4 tumor patients.
In an observational cohort study of 810 laryngeal cancer patients, we evaluated the outcomes of all T4 tumor patients treated with primary chemo-radiotherapy (CRT) or primary radiotherapy alone (RT) compared with upfront total laryngectomy followed by adjuvant (chemo)radiotherapy (TL + a[C]RT). Additionally, we reevaluated the studies that form the evidence base for the recommendation of LP for patients with up to T4 tumors (Pfister et al., J Clin Oncol 24:3693-704, 2006).
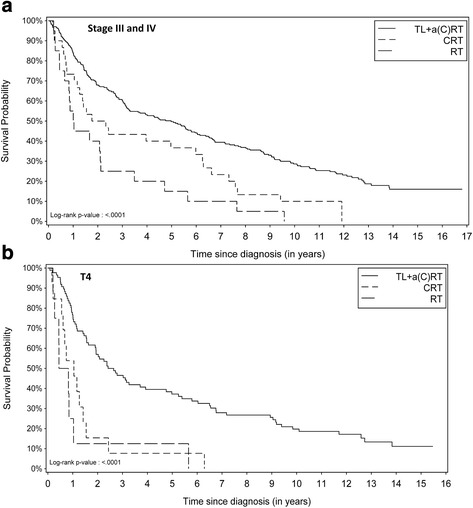
The evaluation of all 288 stage III and IV patients together did not show a significant difference in overall survival (OS) between CRT-LP and TL + a(C)RT (hazard ratio (HR) 1.23; 95% confidence interval (CI): 0.82-1.86; p = 0.31) using a multivariate proportional hazard model. However, a subgroup analysis of T4 tumor patients alone (N = 107; 13.9%) revealed significantly worse OS after CRT compared with TL + a(C)RT (HR 2.0; 95% CI: 1.04-3.7; p = 0.0369). A reevaluation of the subgroup of T4 patients in the 5 LP studies that led to the ASCO clinical practice guidelines revealed that only 21-45 T4 patients had differential data on survival outcome. These data, however, showed a markedly worse outcome for T4 patients after LP.
T4 laryngeal cancer patients who reject TL as a treatment option should be informed that their chance of organ preservation with primary conservative treatment is likely to result in a significantly worse outcome in terms of OS. Significant loss of survival in T4 patients after LP is also confirmed in recent literature.
保留喉(LP)是治疗低体积 T4 喉癌的一种基于证据的治疗选择,它不会影响生存率。然而,对当前文献的重新评估引发了人们对 T4 肿瘤患者是否确实有可靠证据支持保留喉的质疑。
在一项 810 例喉癌患者的观察性队列研究中,我们评估了所有接受原发放化疗(CRT)或单纯放疗(RT)的 T4 肿瘤患者的治疗结果,与直接行全喉切除术加辅助(化疗)放疗(TL+a[C]RT)的结果进行了比较。此外,我们重新评估了构成推荐 T4 肿瘤患者行 LP 证据基础的研究(Pfister 等人,J Clin Oncol 24:3693-704, 2006)。
对所有 288 例 III 期和 IV 期患者进行评估,多变量比例风险模型显示 CRT-LP 与 TL+a(C)RT 在总生存期(OS)方面无显著差异(危险比(HR)1.23;95%置信区间(CI):0.82-1.86;p=0.31)。然而,T4 肿瘤患者亚组分析(N=107;13.9%)显示,CRT 后 OS 明显差于 TL+a(C)RT(HR 2.0;95%CI:1.04-3.7;p=0.0369)。对导致 ASCO 临床实践指南的 5 项 LP 研究中 T4 患者亚组的重新评估表明,只有 21-45 例 T4 患者的生存结果数据存在差异。然而,这些数据显示,T4 患者行 LP 后的结果明显更差。
拒绝 TL 作为治疗选择的 T4 喉癌患者应被告知,他们通过原发保守治疗保留器官的机会可能导致 OS 显著恶化。最近的文献也证实了 T4 患者行 LP 后生存率显著下降。