Fortius Clinic, 17 Fitzhardinge Street, W1H 6EQ, London, UK.
School of Sport, Leeds Beckett University, Leeds, West Yorkshire, UK.
Knee Surg Sports Traumatol Arthrosc. 2017 Dec;25(12):3969-3977. doi: 10.1007/s00167-017-4688-2. Epub 2017 Sep 2.
Adductor longus injuries are complex. The conflict between views in the recent literature and various nineteenth-century anatomy books regarding symphyseal and perisymphyseal anatomy can lead to difficulties in MRI interpretation and treatment decisions. The aim of the study is to systematically investigate the pyramidalis muscle and its anatomical connections with adductor longus and rectus abdominis, to elucidate injury patterns occurring with adductor avulsions.
A layered dissection of the soft tissues of the anterior symphyseal area was performed on seven fresh-frozen male cadavers. The dimensions of the pyramidalis muscle were measured and anatomical connections with adductor longus, rectus abdominis and aponeuroses examined.
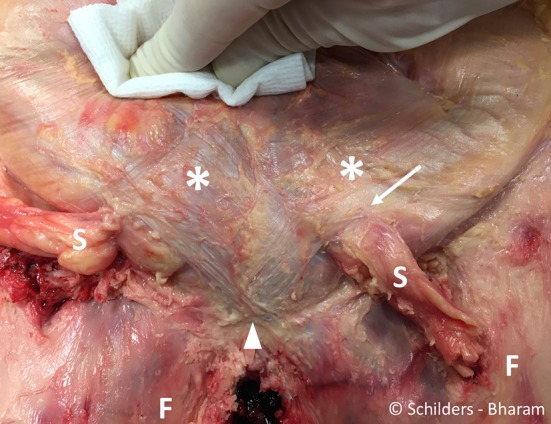
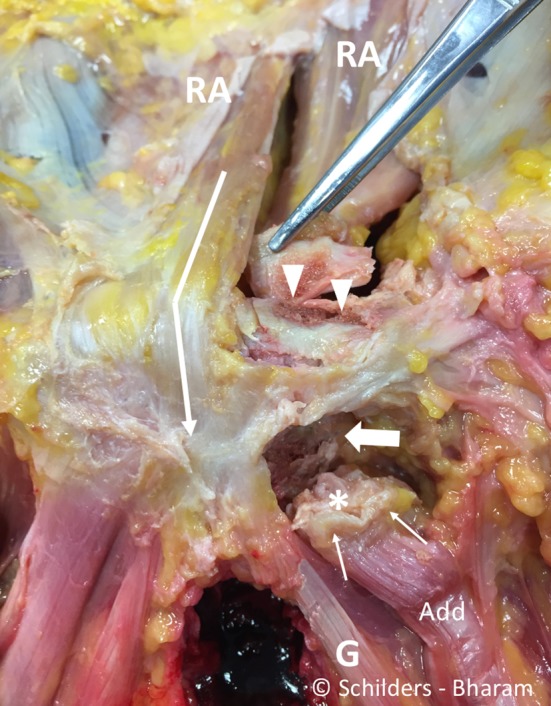
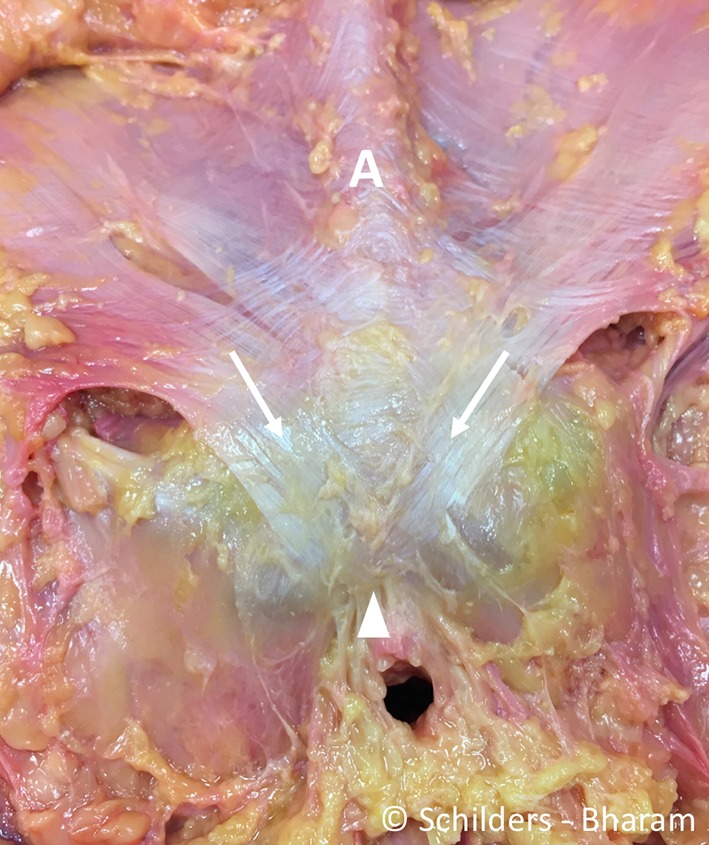
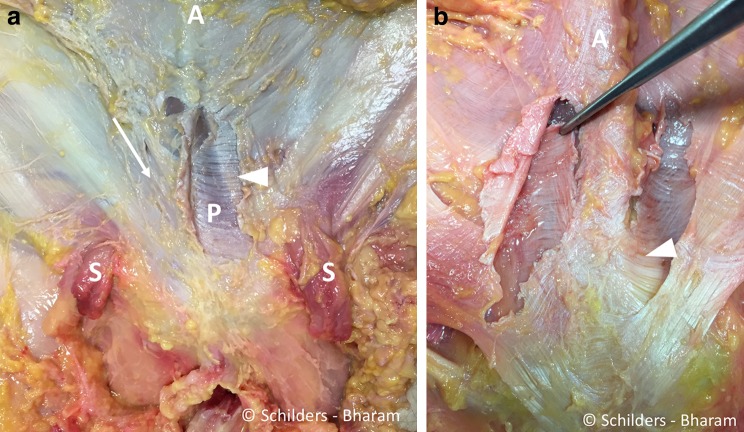
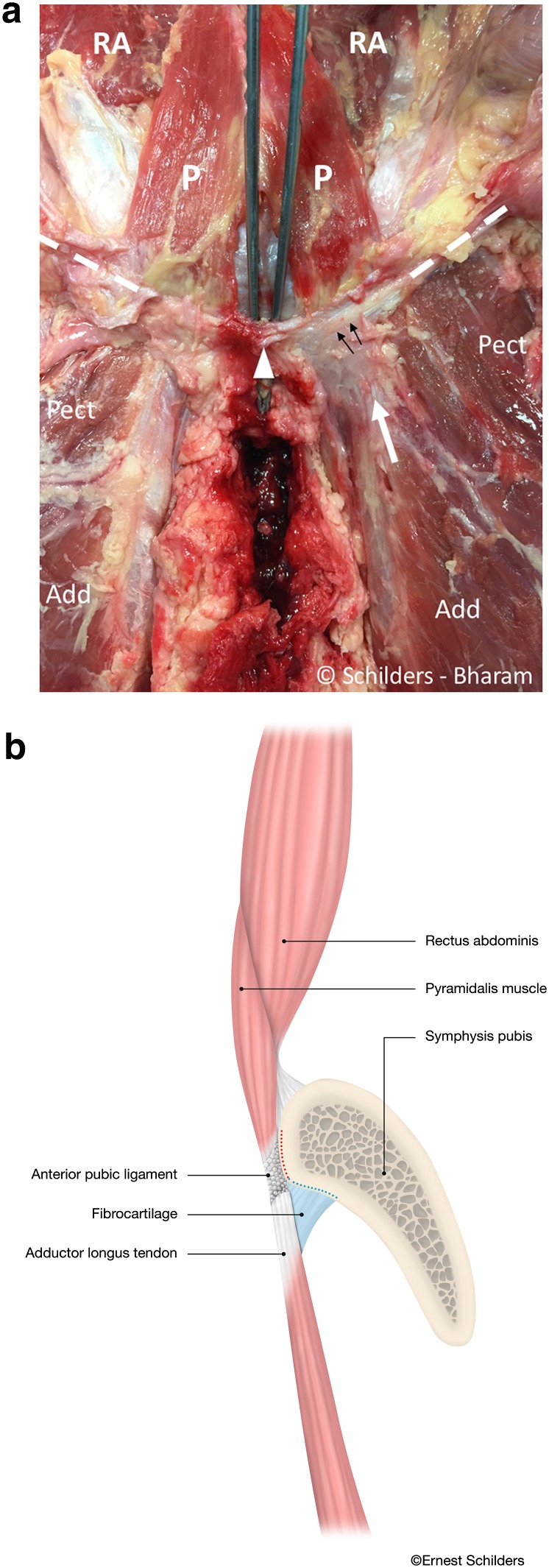
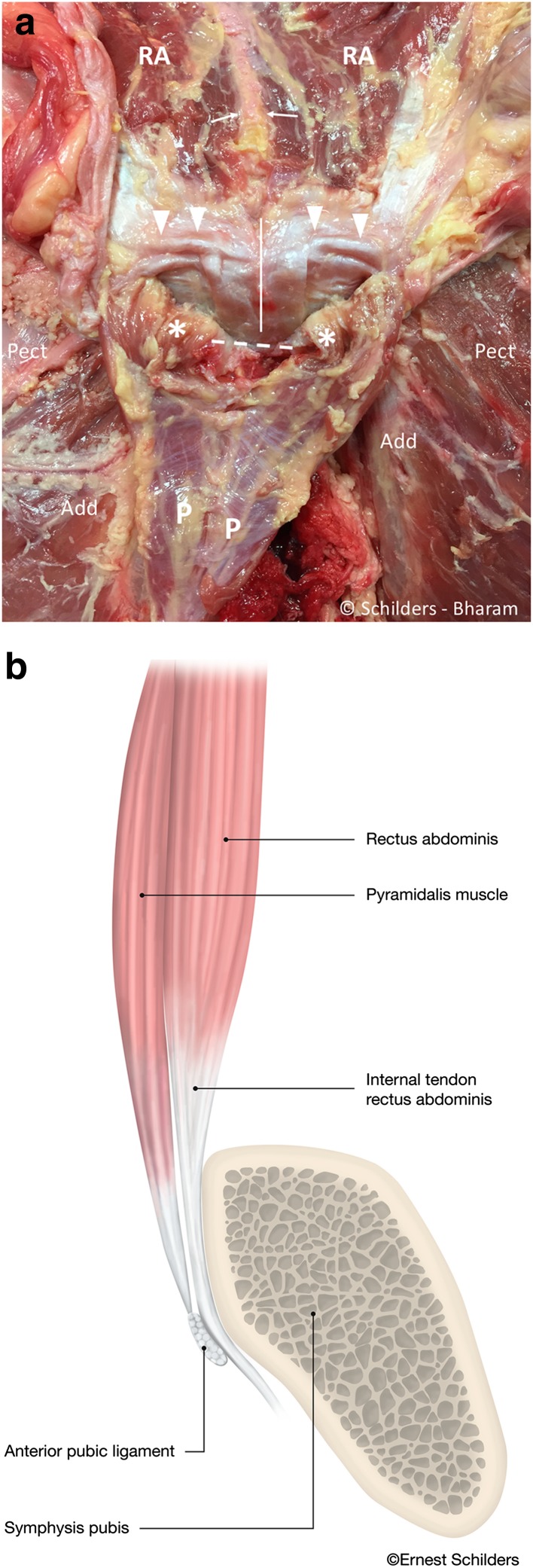
The pyramidalis is the only abdominal muscle anterior to the pubic bone and was found bilaterally in all specimens. It arises from the pubic crest and anterior pubic ligament and attaches to the linea alba on the medial border. The proximal adductor longus attaches to the pubic crest and anterior pubic ligament. The anterior pubic ligament is also a fascial anchor point connecting the lower anterior abdominal aponeurosis and fascia lata. The rectus abdominis, however, is not attached to the adductor longus; its lateral tendon attaches to the cranial border of the pubis; and its slender internal tendon attaches inferiorly to the symphysis with fascia lata and gracilis.
The study demonstrates a strong direct connection between the pyramidalis muscle and adductor longus tendon via the anterior pubic ligament, and it introduces the new anatomical concept of the pyramidalis-anterior pubic ligament-adductor longus complex (PLAC). Knowledge of these anatomical relationships should be employed to aid in image interpretation and treatment planning with proximal adductor avulsions. In particular, MRI imaging should be employed for all proximal adductor longus avulsions to assess the integrity of the PLAC.
内收长肌损伤较为复杂。近期文献中的观点与 19 世纪各种解剖学书籍中关于耻骨联合和耻骨联合周围解剖结构的观点存在冲突,这可能导致 MRI 解读和治疗决策困难。本研究旨在系统研究耻骨肌及其与内收长肌和腹直肌的解剖连接,阐明内收肌撕脱伤的损伤模式。
对 7 具新鲜冷冻男性尸体的前耻骨联合区软组织进行分层解剖。测量耻骨肌的尺寸,并检查其与内收长肌、腹直肌和腱膜的解剖连接。
耻骨肌是耻骨前方唯一的腹肌,在所有标本中均双侧存在。它起自耻骨嵴和耻骨前韧带,止于白线内侧缘。近端内收长肌附着于耻骨嵴和耻骨前韧带。耻骨前韧带也是连接下腹前腱膜和阔筋膜的筋膜附着点。然而,腹直肌并不附着于内收长肌;其外侧腱附着于耻骨头部;其纤细的内侧腱与阔筋膜和股薄肌一起附着于耻骨联合下方。
本研究表明,耻骨肌和内收长肌腱通过耻骨前韧带之间存在强有力的直接连接,并提出了耻骨肌-耻骨前韧带-内收长肌复合体(PLAC)的新概念。了解这些解剖关系有助于辅助近端内收肌撕脱伤的影像学解读和治疗计划。特别是对于所有近端内收长肌撕脱伤,都应采用 MRI 成像来评估 PLAC 的完整性。