Khan Shaukat, Mafara Emma, Pasipamire Munyaradzi, Spiegelman Donna, Mazibuko Sikhathele, Ntshalintshali Nombuso, Hettema Anita, Lejeune Charlotte, Walsh Fiona, Okello Velephi
Clinton Health Access Initiative (CHAI), Mbabane, Swaziland.
Department of Epidemiology, Ministry of Health, Mbabane, Swaziland.
J Int AIDS Soc. 2017 Aug 29;20(Suppl 6):21756. doi: 10.7448/IAS.20.7.21756.
Rapid diagnostic testing has made HIV diagnosis and subsequent treatment more accessible. However, multiple factors, including improper implementation of testing strategies and clerical errors, have been reported to lead to HIV misdiagnosis. The World Health Organization has recommended HIV retesting prior to antiretroviral therapy (ART) initiation which has become pertinent with scaling up of Early Access to ART for All (EAAA). In this analysis, misdiagnosed clients are identified from a subgroup of clients enrolled in EAAA implementation study in Swaziland.
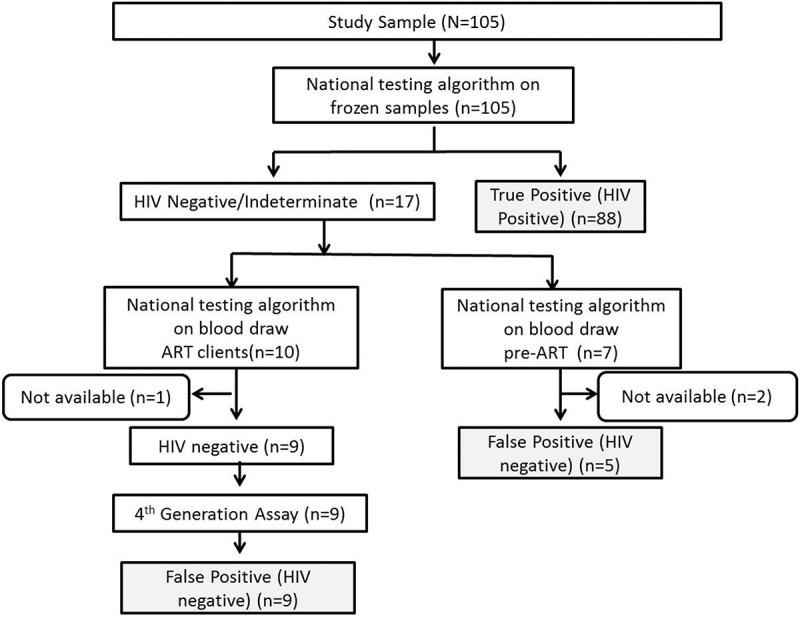
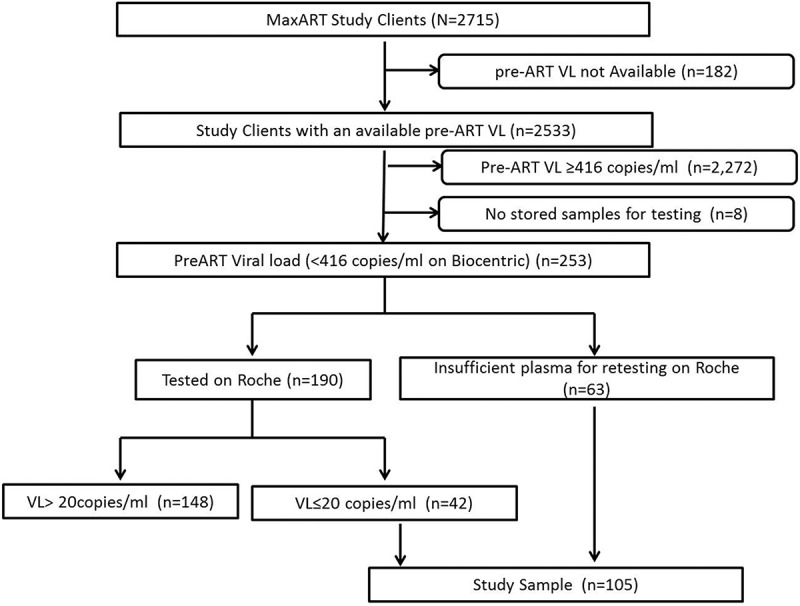
The subgroup to assess misdiagnosis was identified from enrolled EAAA study clients, who had an undetectable viral load prior to ART initiation between September 1, 2014 and May 31, 2016. One hundred and five of 2533 (4%) clients had an undetectable viral load prior to initiation to ART (pre-ART). The HIV status of clients was confirmed using the Determine HIV 1/2 and Uni-Gold HIV 1/2 rapid tests performed serially as recommended by the national testing algorithm. The status of clients on ART was additionally confirmed by fourth-generation HIV Ag/Ab combo tests, Architect and Genscreen Ultra.
Fourteen of the 105 (13%) clients were false positive (HIV negative) on confirmation testing, of whom five (36%) were still in pre-ART care, while nine (64%) were in ART care. Overall, proportion of false positive was 0.6% (14/2533). The false-positive clients had a median CD4 of 791 cells/ml (interquartile range (IQR): 628, 967) compared to 549 cells/ml (IQR: 387, 791) for true positives (HIV positive) ( = 0.0081) and were nearly 20 years older ( = 0.0008).
Overall 0.6% of all enrolled EAAA clients were misdiagnosed, and 64% of misdiagnosed clients were initiated on ART. With adoption of EAAA guidelines by national governments, ART initiation regardless of immunological criteria, strengthening of proficiency testing and adoption of retesting prior to ART initiation would allow identification of misdiagnosed clients and further reduce potential of initiating misdiagnosed clients on ART.
快速诊断检测使艾滋病毒诊断及后续治疗更加便捷。然而,据报道,包括检测策略实施不当和文书错误在内的多种因素会导致艾滋病毒误诊。世界卫生组织建议在开始抗逆转录病毒治疗(ART)之前进行艾滋病毒复检,随着“让所有人尽早获得抗逆转录病毒治疗”(EAAA)的推广,这一点变得至关重要。在本分析中,从斯威士兰参与EAAA实施研究的一组特定客户中识别出误诊客户。
从参与EAAA研究的客户中确定用于评估误诊情况的特定客户组,这些客户在2014年9月1日至2016年5月31日期间开始接受抗逆转录病毒治疗之前病毒载量检测不到。2533名客户中有105名(4%)在开始抗逆转录病毒治疗(ART前)之前病毒载量检测不到。按照国家检测算法的建议,连续使用Determine HIV 1/2和Uni-Gold HIV 1/2快速检测来确认客户的艾滋病毒感染状况。此外,通过第四代艾滋病毒抗原/抗体联合检测、Architect和Genscreen Ultra来确认接受抗逆转录病毒治疗的客户的状况。
105名客户中有14名(13%)在确认检测中为假阳性(艾滋病毒阴性),其中5名(36%)仍处于ART前护理阶段,而9名(64%)正在接受抗逆转录病毒治疗。总体而言,假阳性比例为0.6%(14/2533)。假阳性客户的CD4中位数为791个细胞/毫升(四分位间距(IQR):628,967),而真阳性(艾滋病毒阳性)客户的CD4中位数为549个细胞/毫升(IQR:387,791)(P = 0.0081),且假阳性客户年龄大近20岁(P = 0.0008)。
在所有参与EAAA的客户中,总体有0.6%被误诊,且64%的误诊客户开始接受抗逆转录病毒治疗。随着各国政府采用EAAA指南,无论免疫标准如何都开始进行抗逆转录病毒治疗,加强能力验证并在开始抗逆转录病毒治疗之前采用复检,将能够识别误诊客户,并进一步降低误诊客户开始接受抗逆转录病毒治疗的可能性。