Kufa Tendesayi, Kharsany Ayesha Bm, Cawood Cherie, Khanyile David, Lewis Lara, Grobler Anneke, Chipeta Zawadi, Bere Alfred, Glenshaw Mary, Puren Adrian
Centre for HIV and STIs, National Institutes of Communicable Diseases, Sandringham, South Africa.
School of Public Health, University of the Witwatersrand, Johannesburg, South Africa.
J Int AIDS Soc. 2017 Aug 29;20(Suppl 6):21753. doi: 10.7448/IAS.20.7.21753.
We describe the overall accuracy and performance of a serial rapid HIV testing algorithm used in community-based HIV testing in the context of a population-based household survey conducted in two sub-districts of uMgungundlovu district, KwaZulu-Natal, South Africa, against reference fourth-generation HIV-1/2 antibody and p24 antigen combination immunoassays. We discuss implications of the findings on rapid HIV testing programmes.
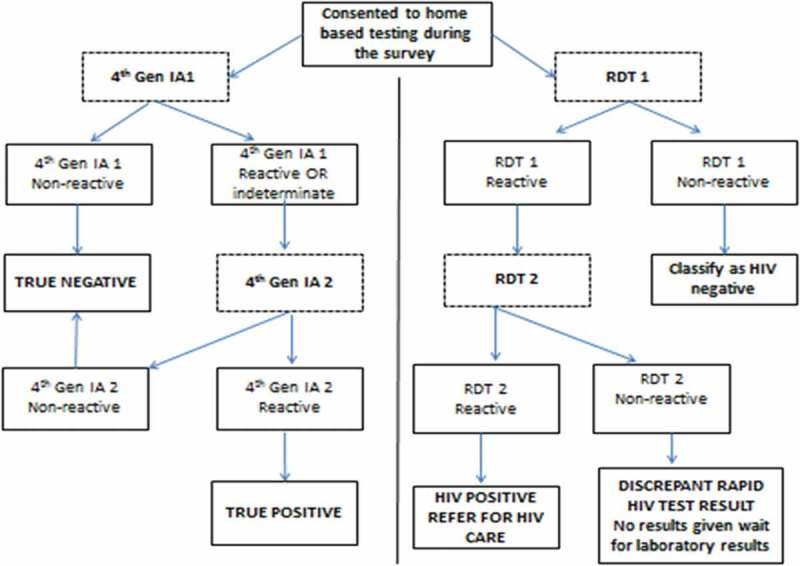
Cross-sectional design: Following enrolment into the survey, questionnaires were administered to eligible and consenting participants in order to obtain demographic and HIV-related data. Peripheral blood samples were collected for HIV-related testing. Participants were offered community-based HIV testing in the home by trained field workers using a serial algorithm with two rapid diagnostic tests (RDTs) in series. In the laboratory, reference HIV testing was conducted using two fourth-generation immunoassays with all positives in the confirmatory test considered true positives. Accuracy, sensitivity, specificity, positive predictive value, negative predictive value and false-positive and false-negative rates were determined.
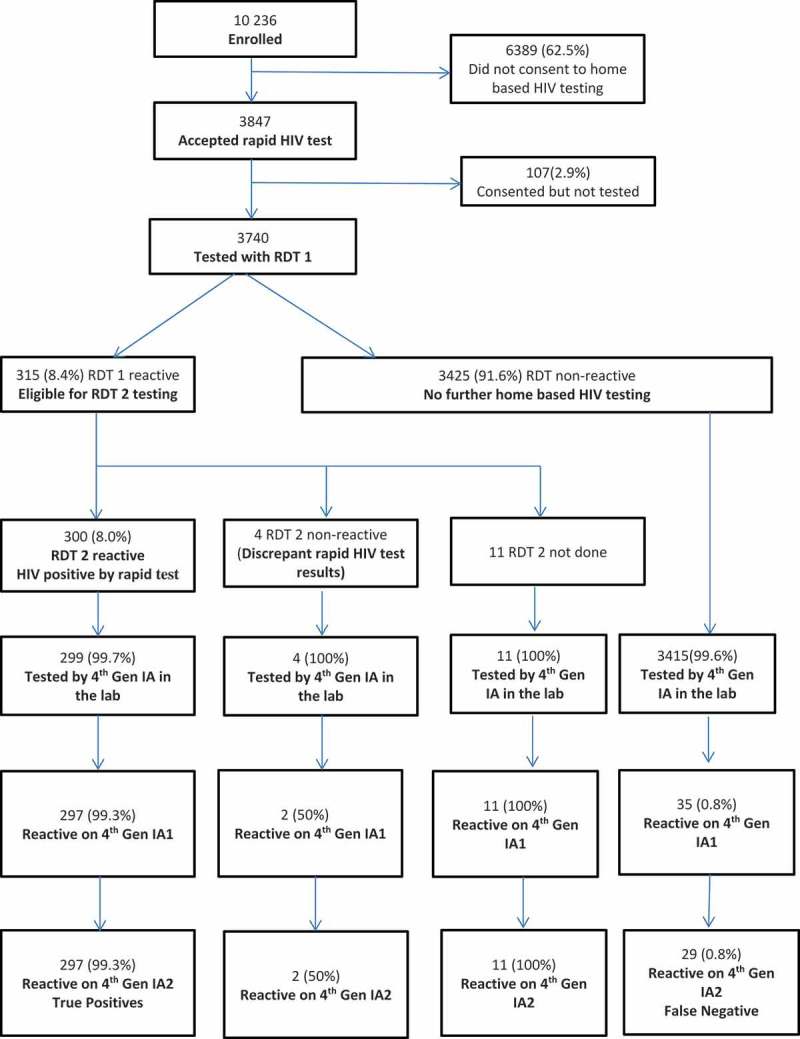
Of 10,236 individuals enrolled in the survey, 3740 were tested in the home (median age 24 years (interquartile range 19-31 years), 42.1% males and HIV positivity on RDT algorithm 8.0%). From those tested, 3729 (99.7%) had a definitive RDT result as well as a laboratory immunoassay result. The overall accuracy of the RDT when compared to the fourth-generation immunoassays was 98.8% (95% confidence interval (CI) 98.5-99.2). The sensitivity, specificity, positive predictive value and negative predictive value were 91.1% (95% CI 87.5-93.7), 99.9% (95% CI 99.8-100), 99.3% (95% CI 97.4-99.8) and 99.1% (95% CI 98.8-99.4) respectively. The false-positive and false-negative rates were 0.06% (95% CI 0.01-0.24) and 8.9% (95% CI 6.3-12.53). Compared to true positives, false negatives were more likely to be recently infected on limited antigen avidity assay and to report antiretroviral therapy (ART) use.
The overall accuracy of the RDT algorithm was high. However, there were few false positives, and the sensitivity was lower than expected with high false negatives, despite implementation of quality assurance measures. False negatives were associated with recent (early) infection and ART exposure. The RDT algorithm was able to correctly identify the majority of HIV infections in community-based HIV testing. Messaging on the potential for false positives and false negatives should be included in these programmes.
在南非夸祖鲁 - 纳塔尔省乌姆贡德洛武区两个分区开展的一项基于人群的家庭调查背景下,我们描述了一种用于社区艾滋病毒检测的连续快速艾滋病毒检测算法相对于参考第四代艾滋病毒1/2抗体和p24抗原联合免疫测定的总体准确性和性能。我们讨论了这些发现对快速艾滋病毒检测项目的影响。
横断面设计:在调查登记后,向符合条件并同意参与的参与者发放问卷,以获取人口统计学和艾滋病毒相关数据。采集外周血样本进行艾滋病毒相关检测。由经过培训的现场工作人员在参与者家中使用包含两个串联快速诊断测试(RDT)的连续算法进行社区艾滋病毒检测。在实验室中,使用两种第四代免疫测定进行参考艾滋病毒检测,确认试验中的所有阳性结果均被视为真阳性。确定准确性、敏感性、特异性、阳性预测值、阴性预测值以及假阳性和假阴性率。
在参与调查的10236人中,3740人在家中接受检测(中位年龄24岁(四分位间距19 - 31岁),42.1%为男性,RDT算法检测出的艾滋病毒阳性率为8.0%)。在接受检测的人中,3729人(99.7%)获得了明确的RDT结果以及实验室免疫测定结果。与第四代免疫测定相比,RDT的总体准确性为98.8%(95%置信区间(CI)98.5 - 99.2)。敏感性、特异性、阳性预测值和阴性预测值分别为91.1%(95% CI 87.5 - 93.7)、99.9%(95% CI 99.8 - 100)、99.3%(95% CI 97.4 - 99.8)和99.1%(95% CI 98.8 - 99.4)。假阳性率和假阴性率分别为0.06%(95% CI 0.01 - 0.24)和8.9%(95% CI 6.3 - 12.53)。与真阳性相比,假阴性在有限抗原亲和力测定中更可能是近期感染,并且更可能报告使用抗逆转录病毒疗法(ART)。
RDT算法的总体准确性较高。然而,尽管实施了质量保证措施,但假阳性较少,且敏感性低于预期,假阴性较高。假阴性与近期(早期)感染和ART暴露有关。RDT算法能够在社区艾滋病毒检测中正确识别大多数艾滋病毒感染。这些项目应纳入关于假阳性和假阴性可能性的信息。