Technau Karl-Günter, Mazanderani Ahmad Haeri, Kuhn Louise, Hans Lucia, Strehlau Renate, Abrams Elaine J, Conradie Martie, Coovadia Ashraf, Mbete Ndileka, Murnane Pamela M, Patel Faeezah, Shiau Stephanie, Tiemessen Caroline T, Sherman Gayle G
Empilweni Services and Research Unit, Department of Paediatrics & Child Health, Rahima Moosa Mother and Child Hospital, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa.
Centre for HIV & STIs, National Institute for Communicable Diseases, Johannesburg, South Africa.
J Int AIDS Soc. 2017 Aug 29;20(Suppl 6):21761. doi: 10.7448/IAS.20.7.21761.
HIV-1 polymerase chain reaction (PCR) testing at birth aims to facilitate earlier initiation of antiretroviral therapy (ART) for HIV-infected neonates. Data from two years of universal birth testing implementation in a high-burden South African urban setting are presented to demonstrate the prevalence and outcomes of diagnostic challenges in this context.
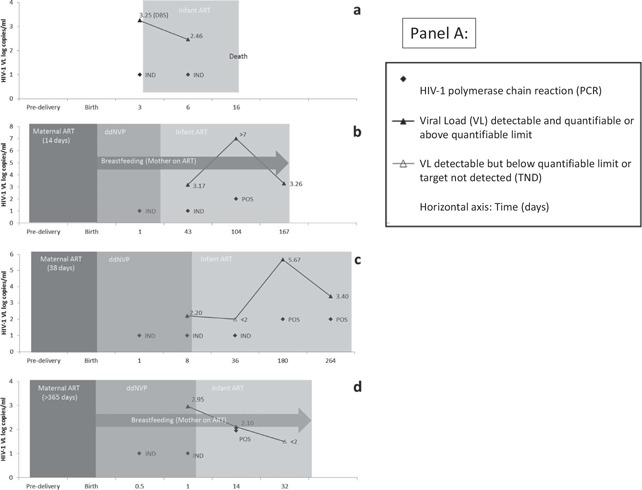
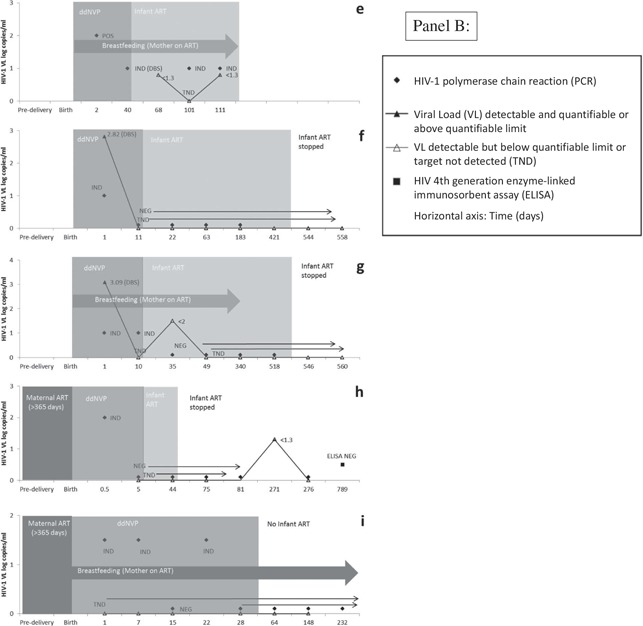
HIV-exposed neonates born at Rahima Moosa Mother and Child Hospital between 5 June 2014 and 31 August 2016 were routinely screened at birth for HIV-1 on whole blood samples using the COBAS® AmpliPrep/COBAS® TaqMan (CAP/CTM) HIV-1 Qualitative Test, version 2.0 (Roche Molecular Systems, Inc., Branchburg, NJ, USA). Virological results were interpreted according to standard operating procedures with the South African National Health Laboratory Service. All neonates with non-negative results were actively followed-up and categorized according to HIV infection status as positive, negative, uncertain and lost to follow-up (LTFU).
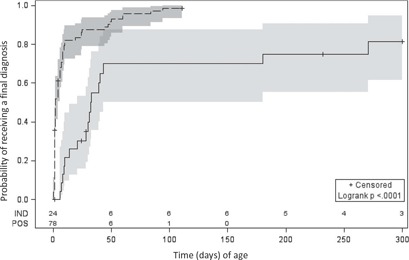
104 (1.8%) of 5743 HIV-exposed neonates received a non-negative birth PCR result, for which laboratory data were available for 102 (98%) cases - 78 (76%) tested positive and 24 (24%) indeterminate. HIV infection status was confirmed positive in 83 (81%) infants, negative in 8 (8%), uncertain in 5 (5%) and LTFU in 6 (6%) cases. The positive predictive value (excluding cases of uncertain diagnosis and inadequate testing) following a non-negative HIV-1 PCR screening test at birth was 0.91 (83/91; 95% confidence interval: 0.85-0.96). Neonates testing positive at birth had significantly higher viral load (VL) results than those testing indeterminate at birth of 4.5 and 3.0 log copies/ml ( = 0.0007), respectively. Similarly, mothers of neonates with positive as compared to indeterminate birth test results had higher VLs of 4.5 and 2.7 log copies/ml ( = 0.0013), respectively. Half of neonates with an indeterminate birth test were shown to be HIV-infected on subsequent confirmatory testing, with time to final diagnosis 30 days longer for these neonates ( < 0.0001).
Indeterminate HIV-1 PCR results accounted for a quarter of non-negative results at birth and were associated with a high risk of infection in comparison to the risk of transmission. Indeterminate birth results with positive HIV PCR results on repeat testing were associated with later final diagnosis. The HIV-1 status remains uncertain in a minority of cases because of repeatedly indeterminate results, highlighting the need for more sensitive and specific virological tests.
出生时进行HIV-1聚合酶链反应(PCR)检测旨在促进对感染HIV的新生儿更早开始抗逆转录病毒治疗(ART)。本文呈现了在南非一个高负担城市环境中开展两年普遍出生检测的数据,以证明在这种情况下诊断挑战的患病率和结果。
2014年6月5日至2016年8月31日在拉希玛·穆萨母婴医院出生的暴露于HIV的新生儿,在出生时使用COBAS® AmpliPrep/COBAS® TaqMan(CAP/CTM)HIV-1定性检测2.0版(美国新泽西州布兰奇堡罗氏分子系统公司)对全血样本进行HIV-1常规筛查。病毒学结果根据南非国家卫生实验室服务的标准操作程序进行解读。所有结果为非阴性的新生儿均被积极随访,并根据HIV感染状况分为阳性、阴性、不确定和失访(LTFU)。
5743例暴露于HIV的新生儿中有104例(1.8%)出生时PCR结果为非阴性,其中102例(98%)有实验室数据——78例(76%)检测呈阳性,24例(24%)结果不确定。83例(81%)婴儿的HIV感染状况被确诊为阳性,8例(8%)为阴性,5例(5%)不确定,6例(6%)失访。出生时HIV-1 PCR筛查检测结果为非阴性后的阳性预测值(不包括诊断不确定和检测不充分的病例)为0.91(83/91;95%置信区间:0.85 - 0.96)。出生时检测呈阳性的新生儿的病毒载量(VL)结果显著高于出生时检测结果不确定的新生儿,分别为4.5和3.0 log拷贝/ml(P = 0.0007)。同样,出生检测结果为阳性的新生儿的母亲与结果不确定的母亲相比,VL分别为4.5和2.7 log拷贝/ml(P = 0.0013)。出生检测结果不确定的新生儿中有一半在后续确诊检测中被证明感染了HIV,这些新生儿最终诊断的时间延长了30天(P < 0.0001)。
HIV-1 PCR结果不确定占出生时非阴性结果的四分之一,与传播风险相比,感染风险较高。重复检测时HIV PCR结果为阳性但出生结果不确定与最终诊断较晚相关。由于结果反复不确定,少数病例的HIV-1状态仍不确定,这突出了需要更敏感和特异的病毒学检测。