Cardiovascular and Pulmonary Branch, Division of Intramural Research, National Heart Lung and Blood Institute, National Institutes of Health, Building 10, Room 2c713, MSC 1538, Bethesda, MD, 20892-1538, USA.
Division of Cardiology, Rady Children's Hospital, 3020 Children's Way, San Diego, CA, 92123, USA.
J Cardiovasc Magn Reson. 2017 Sep 6;19(1):65. doi: 10.1186/s12968-017-0374-2.
Children with heart disease may require repeated X-Ray cardiac catheterization procedures, are more radiosensitive, and more likely to survive to experience oncologic risks of medical radiation. Cardiovascular magnetic resonance (CMR) is radiation-free and offers information about structure, function, and perfusion but not hemodynamics. We intend to perform complete radiation-free diagnostic right heart catheterization entirely using CMR fluoroscopy guidance in an unselected cohort of pediatric patients; we report the feasibility and safety.
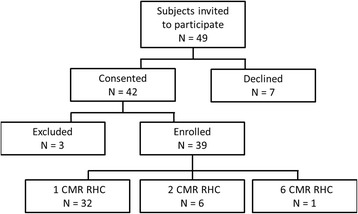
We performed 50 CMR fluoroscopy guided comprehensive transfemoral right heart catheterizations in 39 pediatric (12.7 ± 4.7 years) subjects referred for clinically indicated cardiac catheterization. CMR guided catheterizations were assessed by completion (success/failure), procedure time, and safety events (catheterization, anesthesia). Pre and post CMR body temperature was recorded. Concurrent invasive hemodynamic and diagnostic CMR data were collected.
During a twenty-two month period (3/2015 - 12/2016), enrolled subjects had the following clinical indications: post-heart transplant 33%, shunt 28%, pulmonary hypertension 18%, cardiomyopathy 15%, valvular heart disease 3%, and other 3%. Radiation-free CMR guided right heart catheterization attempts were all successful using passive catheters. In two subjects with septal defects, right and left heart catheterization were performed. There were no complications. One subject had six such procedures. Most subjects (51%) had undergone multiple (5.5 ± 5) previous X-Ray cardiac catheterizations. Retained thoracic surgical or transcatheter implants (36%) did not preclude successful CMR fluoroscopy heart catheterization. During the procedure, two subjects were receiving vasopressor infusions at baseline because of poor cardiac function, and in ten procedures, multiple hemodynamic conditions were tested.
Comprehensive CMR fluoroscopy guided right heart catheterization was feasible and safe in this small cohort of pediatric subjects. This includes subjects with previous metallic implants, those requiring continuous vasopressor medication infusions, and those requiring pharmacologic provocation. Children requiring multiple, serial X-Ray cardiac catheterizations may benefit most from radiation sparing. This is a step toward wholly CMR guided diagnostic (right and left heart) cardiac catheterization and future CMR guided cardiac intervention.
ClinicalTrials.gov NCT02739087 registered February 17, 2016.
患有心脏病的儿童可能需要多次 X 射线心脏导管插入术,对辐射更敏感,并且更有可能存活下来,从而面临医疗辐射的肿瘤风险。心血管磁共振(CMR)无辐射,并提供结构,功能和灌注信息,但不提供血液动力学信息。我们打算在未经选择的儿科患者队列中完全使用 CMR 透视引导进行完全无辐射的诊断性右心导管插入术;我们报告其可行性和安全性。
我们对 39 名儿科患者(12.7 ± 4.7 岁)进行了 50 次 CMR 透视引导的全面经股右心导管插入术,这些患者因临床指征需要进行心脏导管插入术。通过完成(成功/失败),手术时间和安全性事件(导管插入术,麻醉)来评估 CMR 引导的导管插入术。记录 CMR 前后的体温。同时收集有创血液动力学和诊断性 CMR 数据。
在二十两个月的时间内(2015 年 3 月至 2016 年 12 月),入组的患者具有以下临床指征:心脏移植后 33%,分流术 28%,肺动脉高压 18%,心肌病 15%,瓣膜性心脏病 3%,其他 3%。使用被动导管成功完成了所有无辐射的 CMR 引导的右心导管插入术尝试。在两名患有室间隔缺损的患者中,进行了右心和左心导管插入术。没有并发症。一名患者进行了六次此类手术。大多数患者(51%)已进行了多次(5.5 ± 5)次 X 射线心脏导管插入术。保留的胸外科或经导管植入物(36%)不会妨碍 CMR 透视心脏导管插入术的成功进行。在手术过程中,由于心功能差,有两名患者在基线时接受了加压素输注,并且在十次手术中,对多种血液动力学条件进行了测试。
在该小型儿科患者队列中,全面的 CMR 透视引导右心导管插入术是可行且安全的。这包括以前有金属植入物的患者,那些需要持续使用血管加压药输注的患者以及那些需要药物激发的患者。需要多次连续 X 射线心脏导管插入术的儿童可能会从辐射保护中受益最大。这是朝着完全 CMR 引导的诊断(右心和左心)心脏导管插入术和未来的 CMR 引导的心脏介入术迈出的一步。
ClinicalTrials.gov NCT02739087 于 2016 年 2 月 17 日注册。