Cardiovascular Branch, Division of Intramural Research, National Heart, Lung, and Blood Institute, National Institutes of Health, Building 10, Room 2C713, Bethesda, MD, 20892-1538, USA.
J Cardiovasc Magn Reson. 2018 Jun 21;20(1):41. doi: 10.1186/s12968-018-0458-7.
Cardiovascular magnetic resonance (CMR) fluoroscopy allows for simultaneous measurement of cardiac function, flow and chamber pressure during diagnostic heart catheterization. To date, commercial metallic guidewires were considered contraindicated during CMR fluoroscopy due to concerns over radiofrequency (RF)-induced heating. The inability to use metallic guidewires hampers catheter navigation in patients with challenging anatomy. Here we use low specific absorption rate (SAR) imaging from gradient echo spiral acquisitions and a commercial nitinol guidewire for CMR fluoroscopy right heart catheterization in patients.
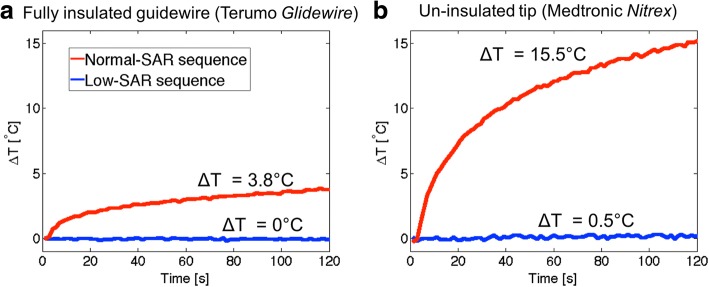
The low-SAR imaging protocol used a reduced flip angle gradient echo acquisition (10° vs 45°) and a longer repetition time (TR) spiral readout (10 ms vs 2.98 ms). Temperature was measured in vitro in the ASTM 2182 gel phantom and post-mortem animal experiments to ensure freedom from heating with the selected guidewire (150 cm × 0.035″ angled-tip nitinol Terumo Glidewire). Seven patients underwent CMR fluoroscopy catheterization. Time to enter each chamber (superior vena cava, main pulmonary artery, and each branch pulmonary artery) was recorded and device visibility and confidence in catheter and guidewire position were scored on a Likert-type scale.
Negligible heating (< 0.07°C) was observed under all in vitro conditions using this guidewire and imaging approach. In patients, chamber entry was successful in 100% of attempts with a guidewire compared to 94% without a guidewire, with failures to reach the branch pulmonary arteries. Time-to-enter each chamber was similar (p=NS) for the two approaches. The guidewire imparted useful catheter shaft conspicuity and enabled interactive modification of catheter shaft stiffness, however, the guidewire tip visibility was poor.
Under specific conditions, trained operators can apply low-SAR imaging and using a specific fully-insulated metallic nitinol guidewire (150 cm × 0.035" Terumo Glidewire) to augment clinical CMR fluoroscopy right heart catheterization.
Clinicaltrials.gov NCT03152773 , registered May 15, 2017.
心血管磁共振(CMR)透视允许在诊断性心导管插入术期间同时测量心脏功能、流量和腔室压力。迄今为止,由于担心射频(RF)诱导加热,商业金属导丝被认为在 CMR 透视时禁忌使用。由于无法使用金属导丝,因此在具有挑战性的解剖结构的患者中,导管导航受到阻碍。在这里,我们使用来自梯度回波螺旋采集的低比吸收率(SAR)成像和商业 Nitinol 导丝进行 CMR 透视右心导管插入术。
低 SAR 成像方案使用减少的翻转角梯度回波采集(10°对比 45°)和较长的重复时间(TR)螺旋读出(10 ms 对比 2.98 ms)。在 ASTM 2182 凝胶体模和尸体动物实验中进行了体外测量,以确保所选导丝(150 cm×0.035" 角尖 Nitinol Terumo Glidewire)无加热。七名患者接受了 CMR 透视导管插入术。记录进入每个腔室(上腔静脉、主肺动脉和每个肺动脉分支)的时间,并使用李克特量表对导管和导丝位置的设备可见性和置信度进行评分。
在所有使用该导丝和成像方法的体外条件下,观察到的加热可忽略不计(<0.07°C)。在患者中,与没有导丝的情况相比,在 100%的尝试中,导丝成功进入每个腔室,而没有进入肺动脉分支。进入每个腔室的时间(p=NS)两种方法相似。导丝赋予导管轴有用的可视性,并能够交互式修改导管轴的刚度,但是导丝尖端的可视性较差。
在特定条件下,经过培训的操作人员可以应用低 SAR 成像,并使用特定的全绝缘金属 Nitinol 导丝(150 cm×0.035" Terumo Glidewire)增强临床 CMR 透视右心导管插入术。
Clinicaltrials.gov NCT03152773,于 2017 年 5 月 15 日注册。