Ferrari Enrico, Eeckhout Eric, Keller Sanjiv, Muller Olivier, Tozzi Piergiorgio, Berdajs Denis, von Segesser Ludwig Karl
Department of Cardiac Surgery, Cardiocentro Ticino Foundation, Via Tesserete 48, 6900, Lugano, Switzerland.
Cardiovascular Research Unit, University Hospital, Lausanne, Switzerland.
J Cardiothorac Surg. 2017 Sep 6;12(1):78. doi: 10.1186/s13019-017-0638-9.
Transcatheter aortic valve implantation is indicated in high-risk patients with aortic stenosis. We compared the clinical outcome of 180 consecutive patients who underwent transapical (TA) and transfemoral (TF) procedures in a single centre.
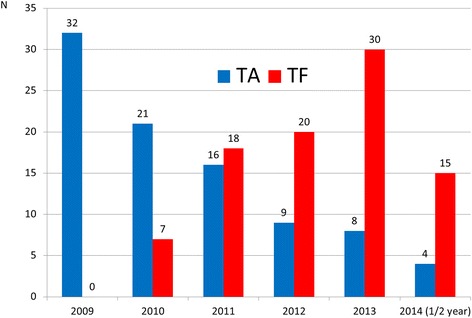
Ninety consecutive TA (TA-group) and 90 consecutive TF (TF-group) were performed from 2009 to 2014. Clinical variables were prospectively collected and retrospectively analysed for hospital outcomes and to identify risk factors for hospital mortality, vascular complications and stroke.
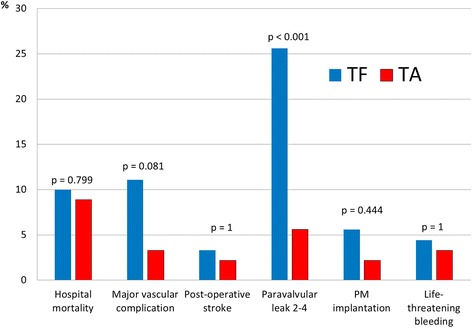
Mean age was 80 ± 8.5 and 83 ± 8.4 years, in the TA and TF-group, respectively. TA-group presented higher prevalence of comorbidities: more vascular disease (79% vs 22%, p < 0.001), chronic pulmonary disease (32% vs 10%, p < 0.001), previous vascular surgery (14% vs 4%, p = 0.039), coronary disease (60% vs 40%, p = 0.007), and previous cardiac surgery (28% vs 17%, p = 0.073). Logistic Euroscore was 36 ± 15% in the TA-group and 25 ± 14% in the TF-group (p < 0.001), but hospital mortality was similar (TA:9%, TF:10%, p = 0.799). Access-related vascular complications occurred more often in transfemoral patients (TA:3%, TF:11%, p = 0.081) while major bleeding (TA:3%, TF:4%, p = 1) and stroke (TA:2%, TF:3%, p = 1) were equally distributed. Postoperative renal failure and dialysis were associated with impaired neurological outcome (p = 0.035 and p = 0.020, respectively). Mild to severe paravalvular leak was more prevalent in transfemoral patients (TA:5%, TF:25%, p < 0.001).
In our experience, the TA and TF-group presented different risk profiles but mortality rate and adverse neurological outcome had a similar incidence. The transfemoral approach carried more vascular complications and paravalvular leaks but last-generation devices will improve this outcome.
经导管主动脉瓣植入术适用于高危主动脉瓣狭窄患者。我们比较了在单一中心连续接受经心尖(TA)和经股动脉(TF)手术的180例患者的临床结局。
2009年至2014年期间,连续进行了90例TA手术(TA组)和90例TF手术(TF组)。前瞻性收集临床变量,并对医院结局进行回顾性分析,以确定医院死亡率、血管并发症和中风的危险因素。
TA组和TF组的平均年龄分别为80±8.5岁和83±8.4岁。TA组合并症的患病率更高:血管疾病更多(79%对22%,p<0.001)、慢性肺病(32%对10%,p<0.001)、既往血管手术史(14%对4%,p=0.039)、冠心病(60%对40%,p=0.007)以及既往心脏手术史(28%对17%,p=0.073)。TA组的逻辑欧洲心脏手术风险评估系统(Logistic Euroscore)为36±15%,TF组为25±14%(p<0.001),但医院死亡率相似(TA组:9%,TF组:10%,p=0.799)。经股动脉手术患者的与穿刺部位相关的血管并发症更常见(TA组:3%,TF组:11%,p=0.081),而大出血(TA组:3%,TF组:4%,p=1)和中风(TA组:2%,TF组:3%,p=1)的分布相同。术后肾衰竭和透析与神经功能结局受损相关(分别为p=0.035和p=0.020)。轻至重度瓣周漏在经股动脉手术患者中更为普遍(TA组:5%,TF组:25%,p<0.001)。
根据我们的经验,TA组和TF组呈现出不同的风险特征,但死亡率和不良神经功能结局的发生率相似。经股动脉手术方法会带来更多的血管并发症和瓣周漏,但新一代装置将改善这一结局。