Miller Joseph B, Arter Andrew, Wilson Suprat S, Janke Alexander T, Brody Aaron, Reed Brian P, Levy Phillip D
Henry Ford Hospital, Department of Emergency Medicine, Detroit, Michigan.
Detroit Medical Center, Detroit Receiving Hospital, Detroit, Michigan.
West J Emerg Med. 2017 Aug;18(5):957-962. doi: 10.5811/westjem.2017.5.33410. Epub 2017 Jul 11.
While moderate to severely elevated blood pressure (BP) is present in nearly half of all emergency department (ED) patients, the incidence of true hypertensive emergencies in ED patients is low. Administration of bolus intravenous (IV) antihypertensive treatment to lower BP in patients without a true hypertensive emergency is a wasteful practice that is discouraged by hypertension experts; however, anecdotal evidence suggests this occurs with relatively high frequency. Accordingly, we sought to assess the frequency of inappropriate IV antihypertensive treatment in ED patients with elevated BP absent a hypertensive emergency.
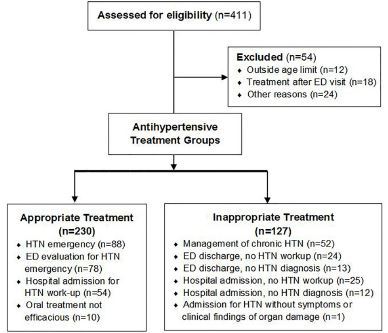
We performed a retrospective cohort study from a single, urban, teaching hospital. Using pharmacy records, we identified patients age 18-89 who received IV antihypertensive treatment in the ED. We defined treatment as inappropriate if documented suspicion for an indicated cardiovascular condition or acute end-organ injury was lacking. Data abstraction included adverse events and 30-day readmission rates, and analysis was primarily descriptive.
We included a total of 357 patients over an 18-month period. The mean age was 55; 51% were male and 93% black, and 127 (36.4%) were considered inappropriately treated. Overall, labetalol (61%) was the most commonly used medication, followed by enalaprilat (18%), hydralazine (18%), and metoprolol (3%). There were no significant differences between appropriate and inappropriate BP treatment groups in terms of clinical characteristics or adverse events. Hypotension or bradycardia occurred in three (2%) patients in the inappropriate treatment cohort and in two (1%) patients in the appropriately treated cohort. Survival to discharge and 30-day ED revisit rates were equivalent.
More than one in three patients who were given IV bolus antihypertensive treatment in the ED received such therapy inappropriately by our definition, suggesting that significant resources could perhaps be saved through education of providers and development of clearly defined BP treatment protocols.
虽然近一半的急诊科患者存在中度至重度血压升高,但急诊科患者中真正的高血压急症发生率较低。在没有真正高血压急症的患者中给予大剂量静脉注射抗高血压治疗以降低血压是一种浪费行为,高血压专家不提倡这种做法;然而,轶事证据表明这种情况发生的频率相对较高。因此,我们试图评估在没有高血压急症的情况下血压升高的急诊科患者中不适当静脉注射抗高血压治疗的频率。
我们在一家城市教学医院进行了一项回顾性队列研究。利用药房记录,我们确定了在急诊科接受静脉注射抗高血压治疗的18至89岁患者。如果缺乏对特定心血管疾病或急性终末器官损伤的记录怀疑,我们将治疗定义为不适当。数据提取包括不良事件和30天再入院率,分析主要是描述性的。
在18个月的时间里,我们共纳入了357名患者。平均年龄为55岁;51%为男性,93%为黑人,127名(36.4%)被认为接受了不适当的治疗。总体而言,拉贝洛尔(61%)是最常用的药物,其次是依那普利拉(18%)、肼屈嗪(18%)和美托洛尔(3%)。在临床特征或不良事件方面,适当和不适当的血压治疗组之间没有显著差异。不适当治疗队列中有3名(2%)患者出现低血压或心动过缓,适当治疗队列中有2名(1%)患者出现这种情况。出院生存率和30天急诊科复诊率相当。
根据我们的定义,在急诊科接受静脉注射大剂量抗高血压治疗的患者中,超过三分之一接受了不适当的治疗,这表明通过对医护人员的教育和制定明确的血压治疗方案,可能可以节省大量资源。