Vuillermoz Cécile, Vandentorren Stéphanie, Brondeel Ruben, Chauvin Pierre
Sorbonne Universités, UPMC Univ Paris 06, INSERM, Institut Pierre Louis d'épidémiologie et de Santé Publique (IPLESP UMRS 1136), Department of Social Epidemiology, Paris, France.
Direction des régions, Santé publique France, Saint Maurice, France.
PLoS One. 2017 Sep 6;12(9):e0184138. doi: 10.1371/journal.pone.0184138. eCollection 2017.
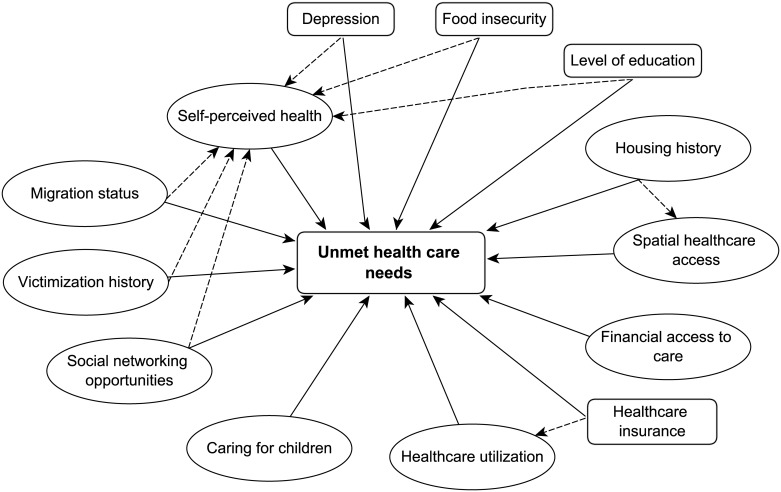
Despite their poor health status, homeless women encounter many barriers to care. The objectives of our study were to estimate the prevalence of unmet healthcare needs in homeless women and to analyse associated relationships with the following factors: financial and spatial access to care, housing history, migration status, healthcare utilisation, victimization history, caring for children, social network and self-perceived health status.
We used data from 656 homeless women interviewed during the ENFAMS representative survey of sheltered homeless families, conducted in the Paris region in 2013. Structural equation models (SEM) were used to estimate the impact of various factors on homeless women's unmet healthcare needs.
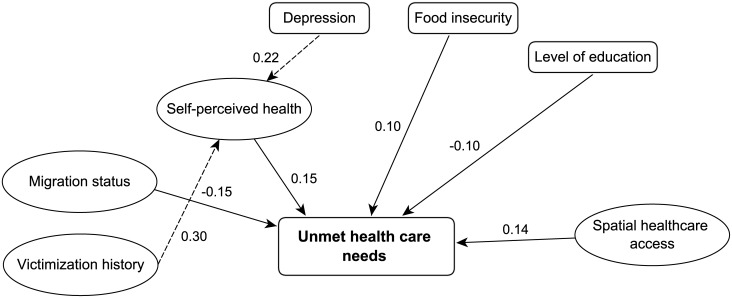
Among those interviewed, 25.1% (95%CI[21.3-29.0]) had at least one unmet healthcare need over the previous year. Most had given up on visiting general practitioners and medical specialists. No association with factors related to financial access or to health insurance status was found. However, food insecurity, poor spatial health access and poor self-perceived health were associated with unmet healthcare needs. Self-perceived health appeared to be affected by victimization and depression.
The lower prevalence of unmet healthcare needs in homeless women compared with women in stable housing situations suggests that homeless women have lower needs perceptions and/or lower expectations of the healthcare system. This hypothesis is supported by the results from SEM. Strategies to provide better access to care for this population should not only focus on financial interventions but also more broadly on spatial healthcare access, cultural norms, and perceptions of health. Reducing their unmet needs and improving their access to healthcare and prevention must include an improvement in their living, financial and housing conditions.
尽管健康状况不佳,但无家可归女性在获得医疗服务方面面临诸多障碍。我们研究的目的是估计无家可归女性未满足的医疗需求的患病率,并分析与以下因素的相关关系:获得医疗服务的经济和空间便利性、住房历史、移民身份、医疗服务利用情况、受害经历、照顾子女情况、社会网络以及自我感知的健康状况。
我们使用了2013年在巴黎地区对有住所的无家可归家庭进行的ENFAMS代表性调查中采访的656名无家可归女性的数据。采用结构方程模型(SEM)来估计各种因素对无家可归女性未满足的医疗需求的影响。
在接受采访的人中,25.1%(95%CI[21.3 - 29.0])在过去一年中至少有一项未满足的医疗需求。大多数人已放弃看全科医生和专科医生。未发现与经济获取或健康保险状况相关的因素有联系。然而,粮食不安全、空间上获得医疗服务的便利性差以及自我感知的健康状况不佳与未满足的医疗需求相关。自我感知的健康状况似乎受到受害经历和抑郁的影响。
与有稳定住房的女性相比,无家可归女性未满足的医疗需求患病率较低,这表明无家可归女性对医疗系统的需求认知较低和/或期望较低。这一假设得到了结构方程模型结果的支持。为这一人群提供更好的医疗服务获取途径的策略不应仅侧重于经济干预,还应更广泛地关注空间上的医疗服务获取、文化规范以及健康认知。减少她们未满足的需求并改善她们获得医疗保健和预防服务的机会,必须包括改善她们的生活、经济和住房条件。