Nimptsch Ulrike, Mansky Thomas
Department for Structural Advancement and Quality Management in Health Care, Technische Universitat Berlin, Berlin, Germany.
BMJ Open. 2017 Sep 6;7(9):e016184. doi: 10.1136/bmjopen-2017-016184.
To explore the existence and strength of a relationship between hospital volume and mortality, to estimate minimum volume thresholds and to assess the potential benefit of centralisation of services.
Observational population-based study using complete German hospital discharge data (Diagnosis-Related Group Statistics (DRG Statistics)).
All acute care hospitals in Germany.
All adult patients hospitalised for 1 out of 25 common or medically important types of inpatient treatment from 2009 to 2014.
Risk-adjusted inhospital mortality.
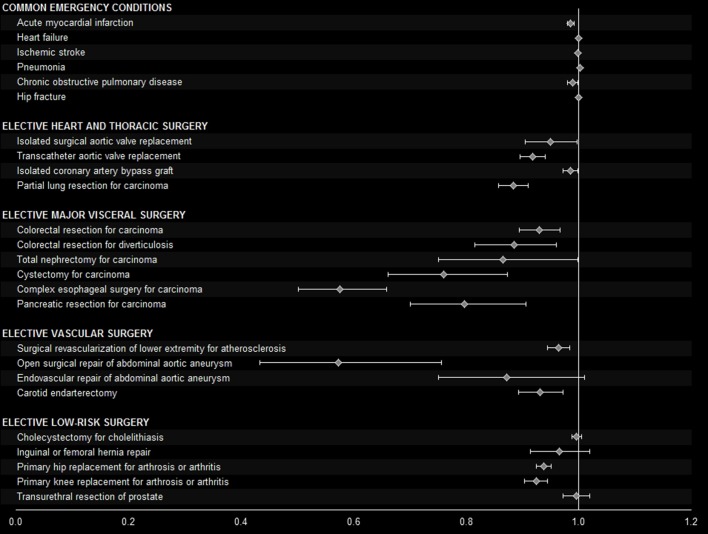
Lower inhospital mortality in association with higher hospital volume was observed in 20 out of the 25 studied types of treatment when volume was categorised in quintiles and persisted in 17 types of treatment when volume was analysed as a continuous variable. Such a relationship was found in some of the studied emergency conditions and low-risk procedures. It was more consistently present regarding complex surgical procedures. For example, about 22 000 patients receiving open repair of abdominal aortic aneurysm were analysed. In very high-volume hospitals, risk-adjusted mortality was 4.7% (95% CI 4.1 to 5.4) compared with 7.8% (7.1 to 8.7) in very low volume hospitals. Theminimum volume above which risk of death would fall below the average mortality was estimated as 18 cases per year. If all hospitals providing this service would perform at least 18 cases per year, one death among 104 (76 to 166) patients could potentially be prevented.
Based on complete national hospital discharge data, the results confirmed volume-outcome relationships for many complex surgical procedures, as well as for some emergency conditions and low-risk procedures. Following these findings, the study identified areas where centralisation would provide a benefit for patients undergoing the specific type of treatment in German hospitals and quantified the possible impact of centralisation efforts.
探讨医院诊疗量与死亡率之间关系的存在性及强度,估计最低诊疗量阈值,并评估服务集中化的潜在益处。
基于德国完整医院出院数据(诊断相关分组统计(DRG统计))的观察性人群研究。
德国所有急性护理医院。
2009年至2014年期间因25种常见或具有医学重要性的住院治疗类型之一而住院的所有成年患者。
风险调整后的住院死亡率。
在25种研究的治疗类型中,当将诊疗量分为五等份时,20种类型中观察到住院死亡率较低与医院诊疗量较高相关,当将诊疗量作为连续变量分析时,17种治疗类型中这种相关性依然存在。在一些研究的急诊情况和低风险手术中发现了这种关系。在复杂外科手术中这种关系更为一致。例如,分析了约22000例接受腹主动脉瘤开放修复术的患者。在高诊疗量医院,风险调整后的死亡率为4.7%(95%可信区间4.1至5.4),而在低诊疗量医院为7.8%(7.1至8.7)。估计每年死亡风险降至平均死亡率以下的最低诊疗量为18例。如果所有提供该服务的医院每年至少进行18例手术,则每104例(76至166例)患者中可能有1例死亡可得到预防。
基于全国完整的医院出院数据,结果证实了许多复杂外科手术以及一些急诊情况和低风险手术中诊疗量与结局之间的关系。根据这些发现,该研究确定了在德国医院中服务集中化对接受特定类型治疗的患者有益的领域,并量化了集中化努力可能产生的影响。