School of Medicine & Dentistry, University of Aberdeen, Aberdeen, UK.
Royal Wolverhampton Hospital, Wolverhampton, UK.
J Am Heart Assoc. 2017 Sep 8;6(9):e006478. doi: 10.1161/JAHA.117.006478.
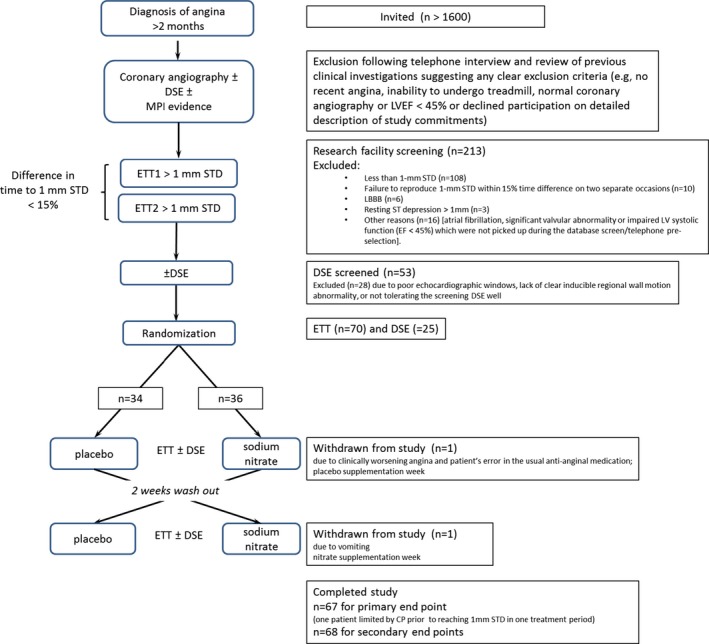
In this double-blind randomized placebo-controlled crossover trial, we investigated whether oral sodium nitrate, when added to existing background medication, reduces exertional ischemia in patients with angina.
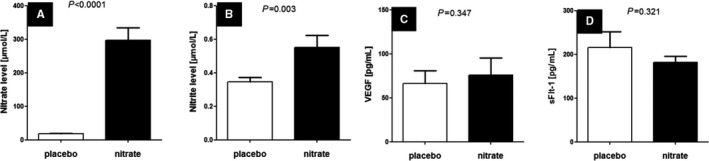
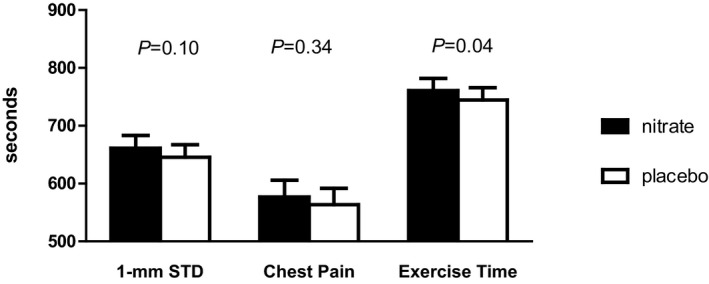
Seventy patients with stable angina, positive electrocardiogram treadmill test, and either angiographic or functional test evidence of significant ischemic heart disease were randomized to receive oral treatment with either placebo or sodium nitrate (600 mg; 7 mmol) for 7 to 10 days, followed by a 2-week washout period before crossing over to the other treatment (n=34 placebo-nitrate, n=36 nitrate-placebo). At baseline and at the end of each treatment, patients underwent modified Bruce electrocardiogram treadmill test, modified Seattle Questionnaire, and subgroups were investigated with dobutamine stress, echocardiogram, and blood tests. The primary outcome was time to 1 mm ST depression on electrocardiogram treadmill test. Compared with placebo, inorganic nitrate treatment tended to increase the primary outcome exercise time to 1 mm ST segment depression (645.6 [603.1, 688.0] seconds versus 661.2 [6183, 704.0] seconds, =0.10) and significantly increased total exercise time (744.4 [702.4, 786.4] seconds versus 760.9 [719.5, 802.2] seconds, =0.04; mean [95% confidence interval]). Nitrate treatment robustly increased plasma nitrate (18.3 [15.2, 21.5] versus 297.6 [218.4, 376.8] μmol/L, <0.0001) and almost doubled circulating nitrite concentrations (346 [285, 405] versus 552 [398, 706] nmol/L, =0.003; placebo versus nitrate treatment). Other secondary outcomes were not significantly altered by the intervention. Patients on antacid medication appeared to benefit less from nitrate supplementation.
Sodium nitrate treatment may confer a modest exercise capacity benefit in patients with chronic angina who are taking other background medication.
URL: https://www.clinicaltrials.gov/. Unique identifier: NCT02078921. EudraCT number: 2012-000196-17.
在这项双盲、随机、安慰剂对照交叉试验中,我们研究了口服硝酸钠在添加到现有基础治疗药物后是否可以减轻心绞痛患者的运动性缺血。
70 名稳定性心绞痛患者,心电图跑步机检查阳性,且存在冠状动脉造影或功能检查明确的缺血性心脏病,随机分为接受安慰剂或硝酸钠(600mg;7mmol)治疗 7-10 天,然后在交叉至另一种治疗方案前洗脱 2 周(n=34 安慰剂-硝酸钠,n=36 硝酸钠-安慰剂)。在基线和每个治疗方案结束时,患者进行改良 Bruce 心电图跑步机测试、西雅图问卷,亚组进行多巴酚丁胺应激、超声心动图和血液检查。主要结局是心电图跑步机试验中 1mmST 段压低的时间。与安慰剂相比,无机硝酸盐治疗组运动至 1mmST 段压低的时间(645.6[603.1,688.0]秒与 661.2[6183,704.0]秒,=0.10)和总运动时间(744.4[702.4,786.4]秒与 760.9[719.5,802.2]秒,=0.04;均值[95%置信区间])均有增加趋势。硝酸盐治疗显著增加了血浆硝酸盐(18.3[15.2,21.5]与 297.6[218.4,376.8]μmol/L,<0.0001),几乎使循环亚硝酸盐浓度增加了一倍(346[285,405]与 552[398,706]nmol/L,=0.003;安慰剂与硝酸盐治疗)。其他次要结局未因干预而显著改变。服用抗酸剂的患者似乎从硝酸盐补充中获益较少。
在服用其他基础治疗药物的慢性心绞痛患者中,口服硝酸钠治疗可能会适度改善运动能力。
网址:https://www.clinicaltrials.gov/。唯一标识符:NCT02078921。EudraCT 编号:2012-000196-17。