Department of Pharmacoepidemiology, Graduate School of Medicine and Public Health, Kyoto University, Yoshida-Konoe-cho, Sakyo-ku, Kyoto, 606-8501, Japan.
Department of Healthcare Epidemiology, Graduate School of Medicine and Public Health, Kyoto University, Yoshida-Konoe-cho, Sakyo-ku, Kyoto, 606-8501, Japan.
BMC Endocr Disord. 2017 Sep 11;17(1):58. doi: 10.1186/s12902-017-0208-0.
Adrenal crisis (AC) occurs in various clinical conditions but previous epidemiological studies in AC are limited to chronic adrenal insufficiency (AI) and sepsis. The aim of this study was to investigate characteristics of AC patients, including predisposing diseases and to describe candidate risk factors for AC such as comorbidities and glucocorticoid (GC) therapy.
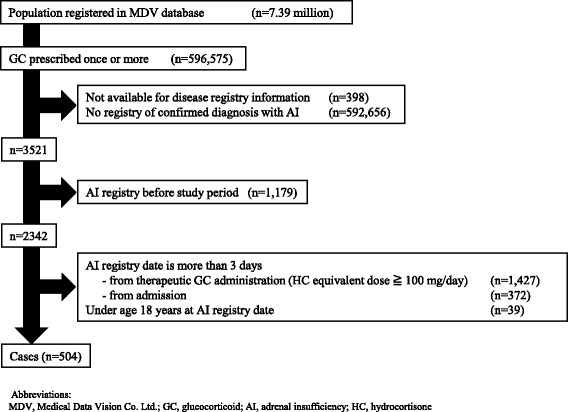
We conducted a retrospective cohort study using a claims database on 7.4 million patients from 145 acute care hospitals between January 1, 2003 and April 30, 2014. We identified AC patients who met the following criteria: 1) disease name with ICD-10 corresponded with AI; 2) therapeutic GC administration (hydrocortisone equivalent dose ≥100 mg/day); 3) admission; and 4) age ≥18 years.
We identified 504 patients with AC (median age, 71 years; interquartile range, 59 to 80; 50.6% male). As predisposing conditions, primary AI and central AI accounted for 23 (4.6%) and 136 patients (27.0%), respectively. In the remaining AC patients (68.5%), comorbidities such as cancer, autoimmune diseases, and renal failure were frequent. The most frequent indication for hospitalization was AC (16.3%), followed by pituitary disease (14.7%), cancer (14.7%), AI-related clinical symptoms (11.5%), and infection (11.1%). Admission under oral GC treatment was reported in 104 patients (20.6%). Twenty-six patients were admitted within 14 days after GC cessation (5.2%).
These findings present an overview of patients with AC in general practice settings, clarifying that predisposing factors for AC were complicated and that patients other than those with chronic AI were older and had more comorbid conditions than those with primary and central AI.
肾上腺危象(AC)可发生于各种临床情况下,但之前有关 AC 的流行病学研究仅限于慢性肾上腺功能不全(AI)和脓毒症。本研究旨在调查 AC 患者的特征,包括易患疾病,并描述 AC 的候选危险因素,如合并症和糖皮质激素(GC)治疗。
我们使用了 2003 年 1 月 1 日至 2014 年 4 月 30 日期间来自 145 家急性护理医院的 740 万患者的索赔数据库进行了回顾性队列研究。我们确定了符合以下标准的 AC 患者:1)疾病名称与 ICD-10 相对应,为 AI;2)给予治疗性 GC 治疗(氢化可的松等效剂量≥100mg/天);3)入院;4)年龄≥18 岁。
我们确定了 504 例 AC 患者(中位数年龄为 71 岁;四分位间距为 59 至 80;50.6%为男性)。作为易患疾病,原发性 AI 和中枢性 AI 分别占 23 例(4.6%)和 136 例(27.0%)。在其余 68.5%的 AC 患者中,常见合并症包括癌症、自身免疫性疾病和肾衰竭。住院的最常见指征是 AC(16.3%),其次是垂体疾病(14.7%)、癌症(14.7%)、与 AI 相关的临床症状(11.5%)和感染(11.1%)。在 104 例患者(20.6%)中报告了口服 GC 治疗的入院。26 例患者在 GC 停药后 14 天内入院(5.2%)。
这些发现概述了普通实践环境中 AC 患者的概况,明确了 AC 的易患因素很复杂,与原发性和中枢性 AI 相比,除了慢性 AI 患者以外,年龄较大且合并症更多的患者患有 AC。