From the, Metabolic Research Laboratories, Wellcome-MRC Institute of Metabolic Science, University of Cambridge, NIHR Cambridge Biomedical Research Centre, Addenbrooke's Hospital, Cambridge, UK.
Centre for Experimental Medicine, Queens University Belfast, Belfast, UK.
J Intern Med. 2021 Aug;290(2):240-256. doi: 10.1111/joim.13273. Epub 2021 Apr 1.
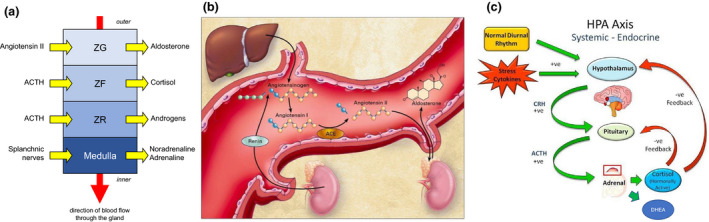
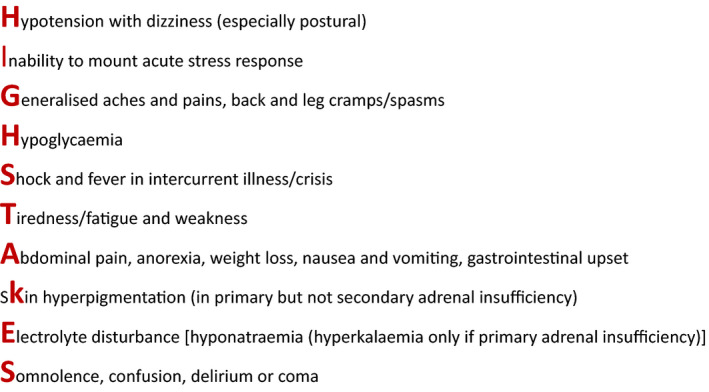
Secondary adrenal insufficiency (AI) occurs as the result of any process that disrupts normal hypothalamic and/or anterior pituitary function and causes a decrease in the secretion of steroid hormones from the adrenal cortex. The most common cause of secondary AI is exogenous corticosteroid therapy administered at supraphysiologic dosages for ≥ 1 month. AI caused by oral corticosteroids (OCS) is not well-recognized or commonly diagnosed but is often associated with reduced well-being and can be life-threatening in the event of an adrenal crisis. Corticosteroid use is common in respiratory diseases, and asthma is a representative condition that illustrates the potential challenges and opportunities related to corticosteroid-sparing therapies. For individuals with severe asthma (approximately 5%-10% of all cases), reduction or elimination of maintenance OCS without loss of control can now be accomplished with biologic therapies targeting inflammatory mediators. However, the optimal strategy to ensure early identification and treatment of AI and safe OCS withdrawal in routine clinical practice remains to be defined. Many studies with biologics have involved short evaluation periods and small sample sizes; in addition, cautious approaches to OCS tapering in studies with a placebo arm, coupled with inconsistent monitoring for AI, have contributed to the lack of clarity. If the goal is to greatly reduce and, where possible, eliminate long-term OCS use in severe asthma through the increasing adoption of biologic treatments, there is an urgent need for clinical trials that address both the speed of OCS withdrawal and how to monitor for AI.
继发性肾上腺功能不全 (AI) 是由于任何破坏下丘脑和/或垂体前叶正常功能的过程引起的,导致肾上腺皮质分泌类固醇激素减少。继发性 AI 的最常见原因是外源性皮质类固醇在生理剂量以上给药 ≥ 1 个月。由口服皮质类固醇 (OCS) 引起的 AI 未得到很好的认识或普遍诊断,但常与幸福感降低有关,在发生肾上腺危象时可能危及生命。皮质类固醇在呼吸系统疾病中很常见,哮喘是一种代表性疾病,说明了与皮质类固醇节约疗法相关的潜在挑战和机遇。对于严重哮喘患者(约占所有病例的 5%-10%),现在可以通过靶向炎症介质的生物疗法来实现不使用维持性 OCS 而控制病情不恶化。然而,在常规临床实践中,确保早期识别和治疗 AI 并安全停用 OCS 的最佳策略仍有待确定。许多生物制剂研究的评估期都较短,样本量也较小;此外,在安慰剂组研究中谨慎地逐渐减少 OCS,并结合对 AI 的不一致监测,导致了这种情况缺乏明确性。如果目标是通过越来越多地采用生物治疗来大大减少和尽可能消除严重哮喘患者的长期 OCS 使用,那么迫切需要进行临床试验,既要解决 OCS 停药的速度,也要解决如何监测 AI 的问题。