Chen Ching-Jen, Ironside Natasha, Pomeraniec I Jonathan, Chivukula Srinivas, Buell Thomas J, Ding Dale, Taylor Davis G, Dallapiazza Robert F, Lee Cheng-Chia, Bergsneider Marvin
Department of Neurological Surgery, University of Virginia Health System, PO Box 800212, Charlottesville, VA, 22908, USA.
Department of Neurosurgery, Auckland City Hospital, Auckland, New Zealand.
Acta Neurochir (Wien). 2017 Nov;159(11):2193-2207. doi: 10.1007/s00701-017-3318-6. Epub 2017 Sep 14.
The aim of this systematic review is to evaluate the long-term endocrine outcomes and postoperative complications following endoscopic vs. microscopic transsphenoidal resection (TSR) for the treatment of acromegaly.
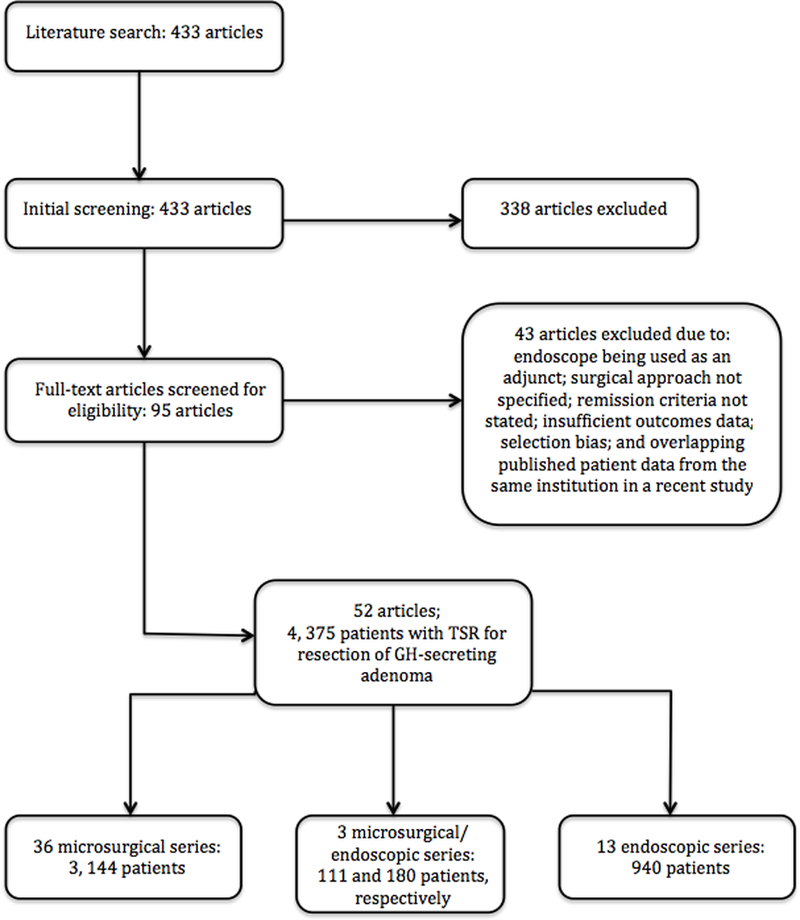
A literature review was performed, and studies with at least five patients who underwent TSR for acromegaly, reporting biochemical remission criteria and long-term remission outcomes were included. Data extracted from each study included surgical technique, perioperative complications, biochemical remission criteria, and long-term remission outcomes.
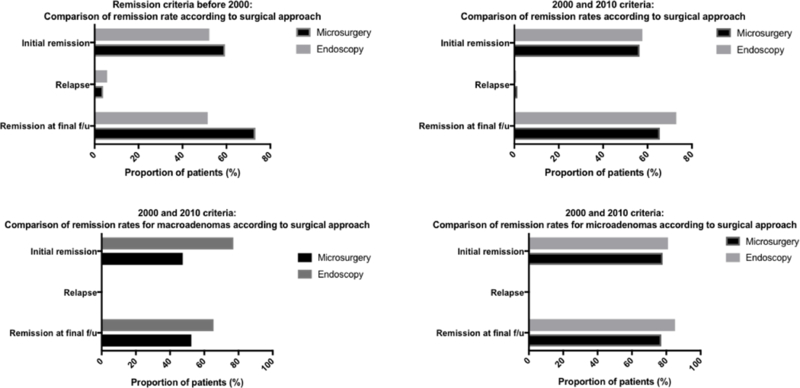
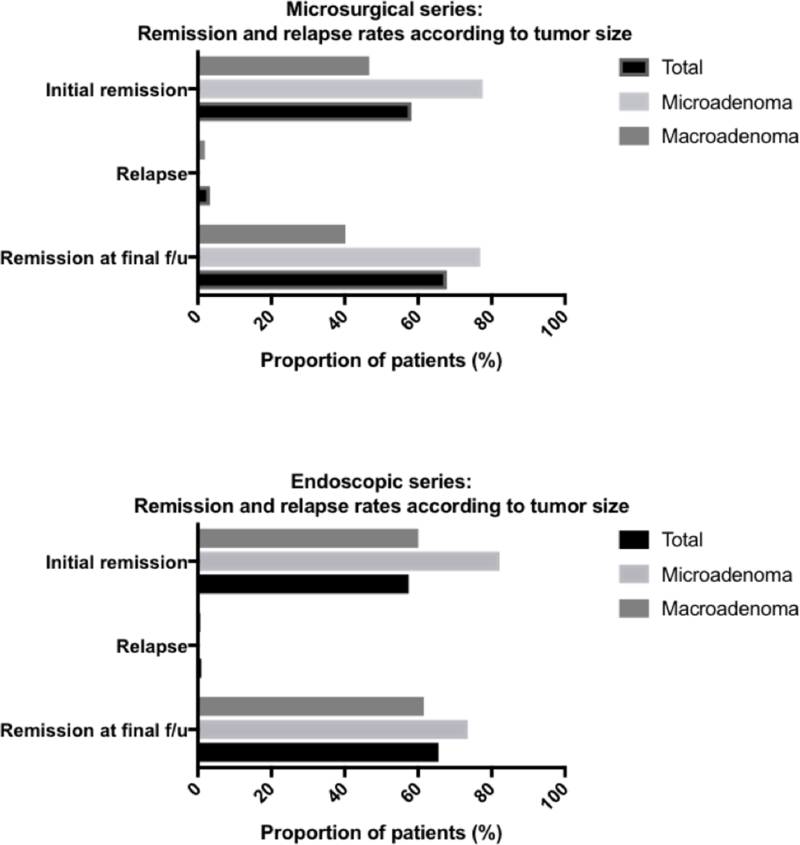
Fifty-two case series from 1976 to 2016 met the inclusion criteria, comprising 4375 patients. Thirty-six reports were microsurgical (n = 3144) and 13 were endoscopic (n = 940). Three studies compared microsurgical (n = 111) to endoscopic TSR outcomes (n = 180). The overall initial and long-term remission rates were 58.2 vs. 57.4% and 69.2 vs. 70.2% for the microsurgical and endoscopic groups, respectively. For microadenomas, the initial and long-term remission rates were 77.6 vs. 82.2% and 76.9 vs. 73.5% for microsurgical and endoscopic approaches, respectively. For macroadenomas, the initial and long-term remission rates were 46.9 vs. 60.0% and 40.2 vs. 61.5% for microsurgical and endoscopic approaches, respectively. The rates of postoperative CSF leak were 3.0 vs. 2.3% for the microscopic and endoscopic groups, respectively. The rates of hypopituitarism and transient diabetes insipidus were 6.7 vs. 6.4% and 9.0 vs. 7.8% for the microscopic and endoscopic groups, respectively.
Both endoscopic and microsurgical approaches for TSR of growth hormone-secreting adenomas are viable treatment options for patients with acromegaly, and yield similarly high rates of remission under the most current consensus criteria.
本系统评价旨在评估内镜与显微镜下经蝶窦切除术(TSR)治疗肢端肥大症后的长期内分泌结局和术后并发症。
进行文献综述,纳入至少有5例接受TSR治疗肢端肥大症患者且报告生化缓解标准和长期缓解结局的研究。从每项研究中提取的数据包括手术技术、围手术期并发症、生化缓解标准和长期缓解结局。
1976年至2016年的52个病例系列符合纳入标准,共4375例患者。36篇报告为显微手术(n = 3144),13篇为内镜手术(n = 940)。3项研究比较了显微手术(n = 111)与内镜TSR结局(n = 180)。显微手术组和内镜手术组的总体初始缓解率和长期缓解率分别为58.2%对57.4%和69.2%对70.2%。对于微腺瘤,显微手术和内镜手术的初始缓解率分别为77.6%对82.2%,长期缓解率分别为76.9%对73.5%。对于大腺瘤,显微手术和内镜手术的初始缓解率分别为46.9%对60.0%,长期缓解率分别为40.2%对61.5%。显微手术组和内镜手术组的术后脑脊液漏发生率分别为3.0%对2.3%。垂体功能减退和短暂性尿崩症的发生率在显微手术组和内镜手术组分别为6.7%对6.4%和9.0%对7.8%。
内镜和显微手术治疗生长激素分泌型腺瘤的TSR方法都是肢端肥大症患者可行的治疗选择,根据最新的共识标准,缓解率同样很高。