FMRIB Centre, University of Oxford, Oxford, UK; Nuffield Division of Anesthetics, Nuffield Department of Clinical Neurosciences, University of Oxford, Oxford, UK.
FMRIB Centre, University of Oxford, Oxford, UK; Nuffield Division of Anesthetics, Nuffield Department of Clinical Neurosciences, University of Oxford, Oxford, UK; School of Psychology and Clinical Language Sciences, University of Reading, UK.
Cortex. 2017 Oct;95:211-221. doi: 10.1016/j.cortex.2017.07.019. Epub 2017 Aug 9.
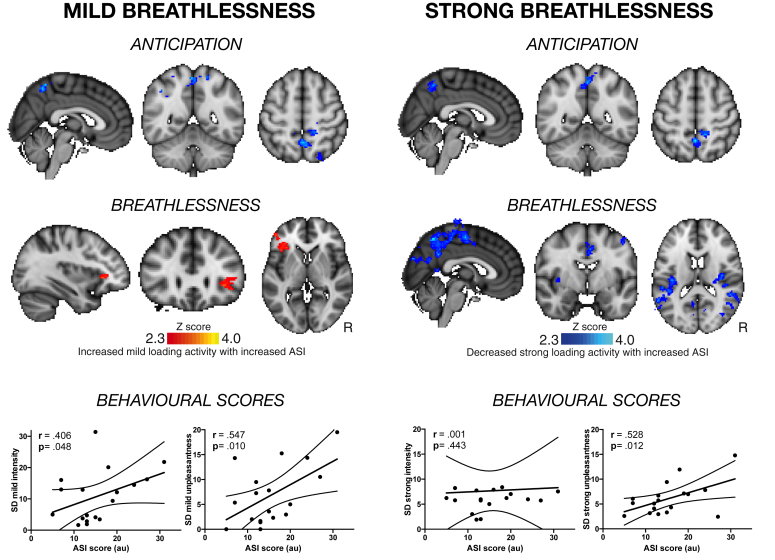
Breathlessness debilitates millions of people with chronic illness. Mismatch between breathlessness severity and objective disease markers is common and poorly understood. Traditionally, sensory perception was conceptualised as a stimulus-response relationship, although this cannot explain how conditioned symptoms may occur in the absence of physiological signals from the lungs or airways. A Bayesian model is now proposed, in which the brain generates sensations based on expectations learnt from past experiences (priors), which are then checked against incoming afferent signals. In this model, psychological factors may act as moderators. They may alter priors, change the relative attention towards incoming sensory information, or alter comparisons between priors and sensations, leading to more variable interpretation of an equivalent afferent input. In the present study we conducted a supplementary analysis of previously published data (Hayen et al., 2017). We hypothesised that individual differences in psychological traits (anxiety, depression, anxiety sensitivity) would correlate with the variability of subjective perceptions of equivalent breathlessness challenges. To better understand the resulting inferential leap in the brain, we explored where these behavioural measures correlated with functional brain activity across subjects. Behaviourally, anxiety sensitivity was found to positively correlate with each subject's variability of intensity and unpleasantness during mild breathlessness, and with variability of unpleasantness during strong breathlessness. In the brain, anxiety sensitivity was found to negatively correlate with precuneus activity during anticipation, positively correlate with anterior insula activity during mild breathlessness, and negatively correlate with parietal sensorimotor areas during strong breathlessness. Our findings suggest that anxiety sensitivity may reduce the robustness of this Bayesian sensory perception system, increasing the variability of breathlessness perception and possibly susceptibility to symptom misinterpretation. These preliminary findings in healthy individuals demonstrate how differences in psychological function influence the way we experience bodily sensations, which might direct us towards better understanding of symptom mismatch in clinical populations.
呼吸困难使数百万患有慢性疾病的人虚弱不堪。呼吸困难的严重程度与客观疾病标志物不匹配的情况很常见,但人们对此了解甚少。传统上,感觉知觉被概念化为一种刺激-反应关系,尽管这并不能解释为什么在没有来自肺部或气道的生理信号的情况下,条件症状可能会出现。现在提出了一种贝叶斯模型,其中大脑根据从过去经验中学习到的期望(先验)产生感觉,然后将这些感觉与传入的感觉信号进行比较。在这个模型中,心理因素可能起调节作用。它们可以改变先验,改变对传入感觉信息的相对关注,或者改变先验与感觉之间的比较,从而导致对等效传入输入的更可变的解释。在本研究中,我们对以前发表的数据(Hayen 等人,2017 年)进行了补充分析。我们假设,心理特征(焦虑、抑郁、焦虑敏感性)的个体差异与对等效呼吸困难挑战的主观感知的可变性相关。为了更好地理解大脑中的推断飞跃,我们探索了这些行为测量与跨受试者的大脑功能活动的相关性。行为上,发现焦虑敏感性与每个受试者在轻度呼吸困难时强度和不愉快的可变性以及在强烈呼吸困难时不愉快的可变性呈正相关。在大脑中,发现焦虑敏感性与预期时的后扣带回活动呈负相关,与轻度呼吸困难时的前岛叶活动呈正相关,与强烈呼吸困难时的顶叶感觉运动区呈负相关。我们的研究结果表明,焦虑敏感性可能会降低这种贝叶斯感觉知觉系统的稳健性,增加呼吸困难知觉的可变性,并可能增加症状误解的易感性。这些在健康个体中的初步发现表明,心理功能的差异如何影响我们体验身体感觉的方式,这可能引导我们更好地理解临床人群中的症状不匹配。