Sung Pei-Hsun, Yang Yao-Hsu, Chiang Hsin-Ju, Chiang John Y, Chen Chi-Jen, Liu Chien-Ting, Yu Cheuk-Man, Yip Hon-Kan
Department of Internal Medicine, Division of Cardiology, Kaohsiung Chang Gung Memorial Hospital and Chang Gung University, College of Medicine, Kaohsiung, Taiwan.
Department of Traditional Chinese Medicine, Chang Gung Memorial Hospital, Chiayi, Taiwan.
Oncotarget. 2017 Mar 17;8(34):57594-57604. doi: 10.18632/oncotarget.16338. eCollection 2017 Aug 22.
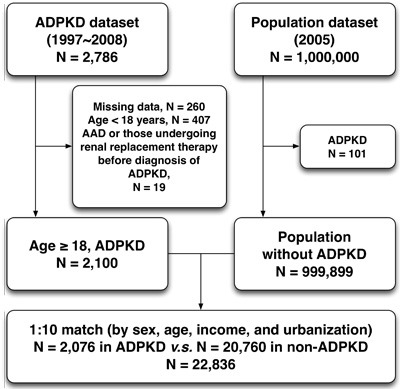
Although cardiovascular complications are the most common cause of death in patients with autosomal-dominant polycystic kidney disease (ADPKD), the incidence and risk of aortic aneurysm and dissection (AAD) in ADPKD remains unclear due to limited data and insufficient cases. We utilized the data from Taiwan National Health Insurance Research Database (NHIRD) to do a population-based cohort study (1997-2008). After excluding those patients with age <18 years old and initially concomitant diagnoses of end-stage renal disease and AAD, a total of 2076 ADPKD patients were selected from 1,000,000 of general population. Additionally, the non-ADPKD group was set up as comparison group in 1:10 ratio after matching with age, gender, income and urbanization (=20760). The result showed that ADPKD group had higher frequency of comorbidities than non-ADPKD group. The frequency of AAD in ADPKD was significantly higher than in general population (0.92% v.s. 0.11%, <0.0001). Of them, 58% of AAD were acute aortic dissection. In addition, Kaplan-Meier analysis demonstrated that cumulative incidence of AAD was remarkably higher in the ADPKD than non-ADPKD group (<0.001). The mean time period from ADPKD diagnosis to AAD occurrence was 4.02±3.16 years. After adjusting for age, gender and comorbidities, the ADPKD patients had up to 5.49-fold greater risk for AAD occurrence as compared to non-ADPKD counterparts (95% CI 2.86-10.52, <0.0001). Particularly, those patients with co-existing ADPKD and hypertension had very high risk for future development of AAD. In conclusion, the risk of AAD significantly increases in patients with ADPKD as compared with those of general population.
尽管心血管并发症是常染色体显性多囊肾病(ADPKD)患者最常见的死亡原因,但由于数据有限且病例不足,ADPKD患者中主动脉瘤和主动脉夹层(AAD)的发病率及风险仍不明确。我们利用台湾全民健康保险研究数据库(NHIRD)的数据进行了一项基于人群的队列研究(1997 - 2008年)。在排除年龄<18岁以及最初伴有终末期肾病和AAD诊断的患者后,从100万普通人群中选取了2076例ADPKD患者。此外,非ADPKD组在按年龄、性别、收入和城市化程度匹配后以1:10的比例设立为对照组(=20760)。结果显示,ADPKD组的合并症发生率高于非ADPKD组。ADPKD患者中AAD的发生率显著高于普通人群(0.92%对0.11%,<0.0001)。其中,58%的AAD为急性主动脉夹层。此外,Kaplan-Meier分析表明,ADPKD组AAD的累积发生率显著高于非ADPKD组(<0.001)。从ADPKD诊断到AAD发生的平均时间为4.02±3.16年。在调整年龄、性别和合并症后,与非ADPKD患者相比,ADPKD患者发生AAD的风险高达5.49倍(95%可信区间2.86 - 10.52,<0.0001)。特别是,同时患有ADPKD和高血压的患者未来发生AAD的风险非常高。总之,与普通人群相比,ADPKD患者发生AAD的风险显著增加。