From the Department of Medicine (Cardiology), New York Harbor Health Care System, Manhattan VA Hospital (B.S.); Department of Medicine (Cardiology), New York University School of Medicine (B.S.); Department of Medicine (Cardiology), Icahn School of Medicine at Mount Sinai, New York, NY (U.B., A.S.K., G.D., M.B.A., S.S., R.M.); Medical Statistics, London School of Hygiene and Tropical Medicine, United Kingdom (S.J.P., C.A.); Department of Medicine (Cardiology), Duke University School of Medicine, Durham, NC (M.W.K.); Department of Medicine (Cardiology), Harvard Medical School, Cambridge, MA (C.M.G.); Department of Medicine (Cardiology), Hôpital Bichat-Claude Bernard, Paris, France (P.G.S.); Department of Medicine (Cardiology), Columbia University Medical Center, New York, NY (G.W.); Department of Medicine (Cardiology), HELIOS Amper-Klinikum Dachau, Germany (B.W.); Department of Medicine (Cardiology), Cedars-Sinai Heart Institute, Los Angeles, CA (T.D.H.); Department of Medicine (Cardiology), Minneapolis Heart Institute Foundation, University of Minnesota (T.D.H.); Department of Medicine (Cardiology), Moses Cone Heart and Vascular Center, LeBauer Cardiovascular Research Foundation, Greensboro, NC (T.S.); Department of Medicine (Cardiology), St Luke's Mid America Heart Institute, University of Missouri-Kansas City (D.J.C.); Department of Medicine (Cardiology), Onassis Cardiac Surgery Center, Athens, Greece (I.I.); Department of Medicine (Cardiology), San Raffaele Hospital, Milan, Italy (A. Chieffo, A. Colombo); and Department of Medicine (Cardiology), University of Kentucky, Lexington (D.J.M.).
Circ Cardiovasc Interv. 2017 Sep;10(9). doi: 10.1161/CIRCINTERVENTIONS.117.004981.
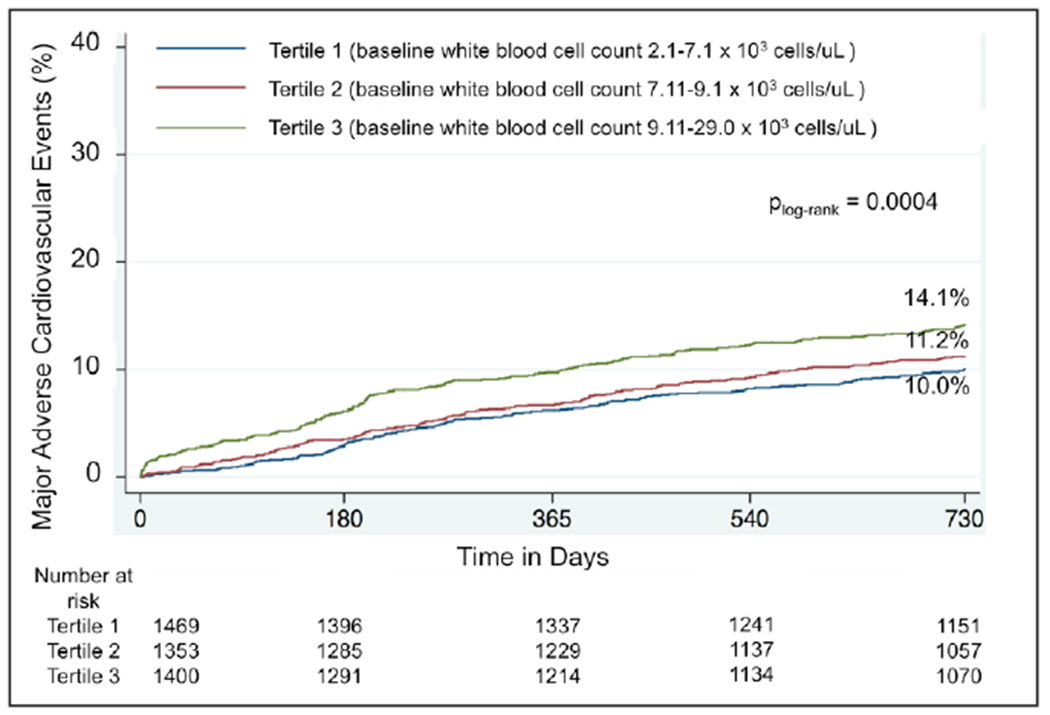
Elevated white blood cell (WBC) count is associated with increased major adverse cardiovascular events (MACE) in the setting of acute coronary syndrome. The aim of this study was to evaluate whether similar associations persist in an all-comers population of patients undergoing percutaneous coronary intervention in the contemporary era.
In the multicenter, prospective, observational PARIS study (Patterns of Non-Adherence to Anti-Platelet Regimens in Stented Patients Registry), 4222 patients who underwent percutaneous coronary intervention in the United States and Europe between July 1, 2009, and December 2, 2010, were evaluated. The associations between baseline WBC and MACE (composite of cardiac death, stent thrombosis, spontaneous myocardial infarction, or target lesion revascularization) at 24-month follow-up were analyzed using multivariable Cox regression. Patients with higher WBC were more often younger, smokers, and with less comorbid risk factors compared with those with lower WBC. After adjustment for baseline and procedural characteristics, WBC remained independently associated with MACE (hazard ratio [HR] per 10 cells/μL increase, 1.05 [95% confidence intervals (CI), 1.02-1.09]; =0.001), cardiac death (HR, 1.10 [95% CI, 1.05-1.17]; <0.001), and clinically indicated target revascularization (HR, 1.04 [95% CI, 1.00-1.09]; =0.03) but not stent thrombosis (HR, 1.07 [95% CI, 0.99-1.16]; =0.10) or spontaneous myocardial infarction (HR, 1.03 [95% CI, 0.97-1.09]; =0.29). The association between WBC and MACE was consistent in acute coronary syndrome and non-acute coronary syndrome presentations (interaction =0.15).
Increased WBC is an independent predictor of MACE after percutaneous coronary intervention in a contemporary all-comers cohort. Further studies to delineate the underlying pathophysiologic role of elevated WBC across a spectrum of coronary artery disease presentations are warranted.
URL: http://www.clinicaltrials.gov. Unique identifier: NCT00998127.
在急性冠状动脉综合征患者中,白细胞计数升高与主要不良心血管事件(MACE)增加相关。本研究旨在评估在当代经皮冠状动脉介入治疗的所有患者中是否存在类似的相关性。
在多中心、前瞻性、观察性 PARIS 研究(接受支架治疗患者的非抗血小板治疗方案依从性模式登记研究)中,评估了 2009 年 7 月 1 日至 2010 年 12 月 2 日期间在美国和欧洲接受经皮冠状动脉介入治疗的 4222 例患者。使用多变量 Cox 回归分析基线白细胞计数与 24 个月随访时 MACE(包括心源性死亡、支架血栓形成、自发性心肌梗死或靶病变血运重建)之间的相关性。与白细胞计数较低的患者相比,白细胞计数较高的患者更年轻、吸烟且合并症风险因素较少。在校正基线和手术特征后,白细胞计数仍与 MACE 独立相关(每增加 10 个/μL,风险比 [HR] 为 1.05 [95%置信区间 [CI],1.02-1.09];=0.001)、心源性死亡(HR,1.10 [95%CI,1.05-1.17];<0.001)和临床指示的靶血管血运重建(HR,1.04 [95%CI,1.00-1.09];=0.03),但与支架血栓形成(HR,1.07 [95%CI,0.99-1.16];=0.10)或自发性心肌梗死(HR,1.03 [95%CI,0.97-1.09];=0.29)无关。白细胞计数与 MACE 之间的相关性在急性冠状动脉综合征和非急性冠状动脉综合征患者中一致(交互作用=0.15)。
在当代所有患者队列中,白细胞计数升高是经皮冠状动脉介入治疗后 MACE 的独立预测因素。需要进一步研究以阐明在一系列冠状动脉疾病患者中升高的白细胞计数的潜在病理生理作用。