Sarfo Fred Stephen, Ovbiagele Bruce, Akassi John, Kyem Gloria
Kwame Nkrumah University of Science & Technology, Kumasi, Ghana.
Komfo Anokye Teaching Hospital, Kumasi, Ghana.
eNeurologicalSci. 2017 Mar;6:68-73. doi: 10.1016/j.ensci.2016.12.003. Epub 2016 Dec 28.
There is a paucity of data on persistence of secondary prevention medications among stroke survivors in resource-limited settings where stroke is on a rapid upward trajectory and its management severely challenged. To avert new cardiovascular events after stroke, preventive medications should be promptly instituted and used continuously. We report 1-year rates and determinants of persistent utilization of secondary prevention therapies after stroke in Ghana.
A retrospective observational study involving 418 stroke survivors enrolled into a Neurology clinic in a tertiary institution in central Ghana between January 2011 and December 2013. Data on demography, stroke type, risk factor profile and five secondary risk prevention medication classes namely antihypertensive, antiplatelet, statins, antidiabetic and anticoagulants were collected from patient charts. Persistence within first year after stroke was defined as continuation of all secondary preventive medications prescribed at enrollment to the Neurology clinic and it excluded 126 (≈30%) patients who could not complete 12 month follow up. Data was closed for analysis in June 2015 to allow for at least 12 months of follow-up.
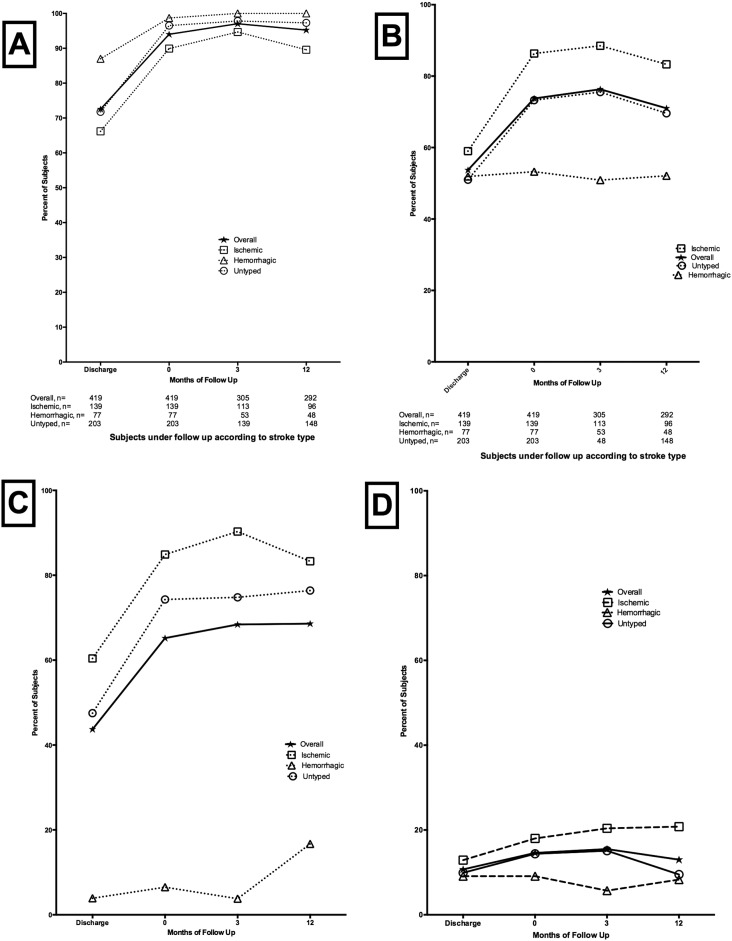
Rates of utilization of secondary preventive medications and its intensity were influenced by stroke type and prevailing vascular risk factors. In decreasing order, antihypertensive, lipid-modifying, anti-platelet, anti-diabetic medications and anti-coagulants were prescribed at frequencies (%) of 394 (94.3%), 303 (72.5%), 274 (65.6%), 61 (14.6%) and 2 (0.5%) respectively at enrollment into the Neurology clinic (n=418). Overall, 92.1% of subjects (n=292) under follow-up for 1 year were persistent on secondary prevention medications initiated at enrollment into the neurology clinic with medication class specific rates of 97.5% for antihypertensive, 94.8% for anti-platelets, 94.1% for statins, 85.7% for anti-diabetic and 50% for anticoagulants. Abuse of alcohol was significantly associated with non-persistence, adjusted OR (95% CI) of 3.08 (1.13-8.38).
Persistence of secondary preventive medications among stroke survivors in this resource-limited setting is excellent and comparable to those in resource-replete countries. There is however the need to investigate the causes of high attrition rates from care.
在资源有限的环境中,中风发病率呈快速上升趋势且管理面临严峻挑战,关于中风幸存者二级预防药物持续性的数据匮乏。为避免中风后发生新的心血管事件,应及时启动并持续使用预防性药物。我们报告了加纳中风后二级预防治疗持续使用的1年发生率及决定因素。
一项回顾性观察研究,纳入了2011年1月至2013年12月期间在加纳中部一所三级医疗机构的神经科诊所登记的418名中风幸存者。从患者病历中收集人口统计学、中风类型、危险因素概况以及五类二级风险预防药物的数据,即抗高血压药、抗血小板药、他汀类药物、抗糖尿病药和抗凝药。中风后第一年内的持续性定义为继续使用在进入神经科诊所时所开的所有二级预防药物,排除了126名(约30%)无法完成12个月随访的患者。数据于2015年6月截止进行分析,以确保至少有12个月的随访期。
二级预防药物的使用率及其强度受中风类型和主要血管危险因素的影响。按降序排列,在进入神经科诊所时(n = 418),抗高血压药、调脂药、抗血小板药、抗糖尿病药和抗凝药的处方频率(%)分别为394(94.3%)、303(72.5%)、274(65.6%)、61(14.6%)和2(0.5%)。总体而言,在接受1年随访的受试者中(n = 292),92.1%的人持续使用在进入神经科诊所时开始的二级预防药物,各类药物的持续使用率分别为:抗高血压药97.5%、抗血小板药94.8%、他汀类药物94.1%、抗糖尿病药85.7%、抗凝药50%。酗酒与持续性显著相关,调整后的比值比(95%可信区间)为3.08(1.13 - 8.38)。
在这种资源有限的环境中,中风幸存者二级预防药物的持续性良好,与资源丰富国家相当。然而,有必要调查护理中高损耗率的原因。