Zdziarski Przemyslaw, Gamian Andrzej, Majda Jacek, Korzeniowska-Kowal Agnieszka
Department of Clinical Immunology, Lower Silesian Center for Cellular Transplantation, POBox 1818, 50-385 Wrocław-46, Poland.
Department of Immunology of Infectious Diseases, Hirszfeld Institute of Immunology and Experimental Therapy, Polish Academy of Sciences, POBox 1818, 50-385 Wrocław-46, Poland.
Allergy Asthma Clin Immunol. 2017 Sep 15;13:41. doi: 10.1186/s13223-017-0213-x. eCollection 2017.
Allergic, especially anaphylactic, reactions during immunoglobulin replacement therapy are rare, but their pathophysiology and classification remain ambiguous. Recent findings show positive results of skin tests with commercially available immunoglobulins, but target antigens and responsible compounds of the tested immunoglobulins have not been strictly identified.
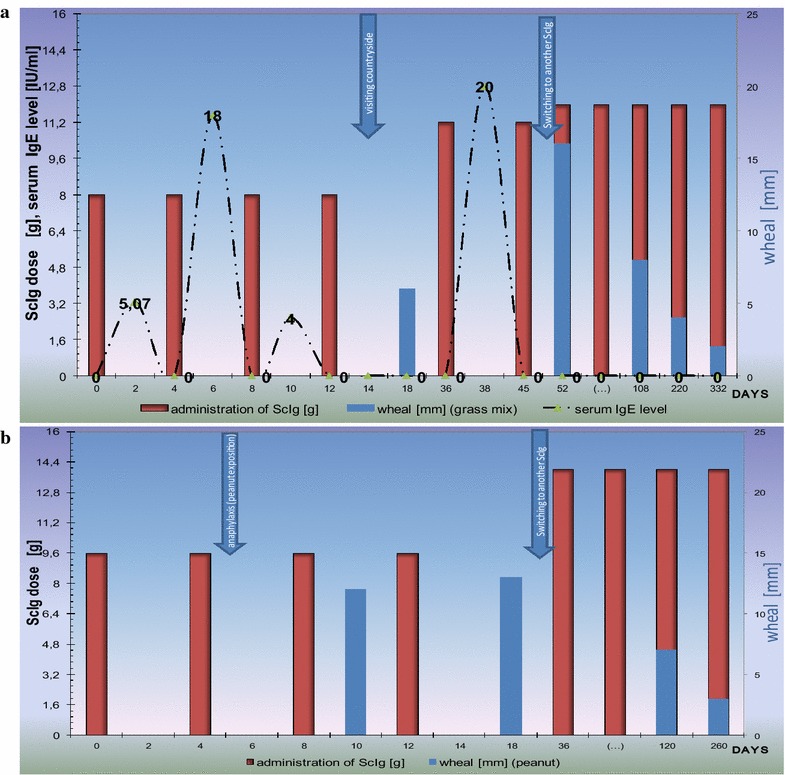
Four adult patients with recently diagnosed common variable immunodeficiency qualified for standard subcutaneous immunoglobulin replacement therapy regimen. They had no history of receiving immunoglobulins, blood or blood product transfusions. Edema, confluent wheals and erythema were observed at the site of subcutaneous immunoglobulin infusion: typical early and late phase reaction. A transient increase in various passively transferred IgG and IgE antibodies was responsible for misleading positive outcome of the serological testing for active humoral response such as type I allergy, anti-Rh, isohemagglutinins and rheumatoid factor (RF). Although the clinical presentation was very unusual and severe, the retrospective analysis showed no isohemagglutinins, RF and IgE in the patients' serum before but it was positive after the infusion (median IgE = 18 IU/ml, RF = 8 IU/ml). Type I allergic reaction (laryngeal edema, rhinoconjuctivitis) came out at +14 days of replacement therapy when the patient visited countryside. In the second patient anaphylactic reaction was observed 5 days after ScIg administration, and only when the patient consumed peanuts. Therefore, IgE concentration was measured retrospectively in a series of commercial preparations used in the initial subcutaneous immunoglobulin replacement therapy that caused the adverse event (AE) and it was determined between 138 and 232 IU/ml (kU/l), i.e. 690-2100 IU per g of protein. Specific IgE was within a wide range from 198 (mix of food) to 2809 kUA/l (mix of grass) but many of the tested allergen-specific IgE were class 2 or 3 (i.e. 0.71-17.5 kUA/l).
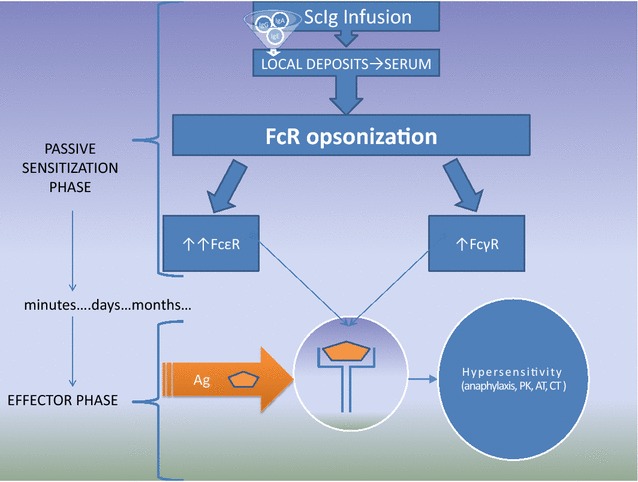
The case resembles passive cutaneous anaphylaxis and Prausnitz-Küstner reaction but clinical significance of the classical phenomena has not yet been described. This observation indicates that anaphylactic reactions during immunoglobulin replacement therapy may result from IgE or pathological IgG content. Such IgE presence was sporadically reported (34.5-105 IU/ml, i.e. 862.5-1450 IU/g of protein) in intravenous immunoglobulins that are used and monitored by healthcare professionals. In clinical practice the definition of adverse events is inadequate since individual batches of immunoglobulins come with different specificity therefore, they should be classified as transfusion products (not bioequivalents). Such new approach implies establishing (1) new control methods and strategies to ensure introduction of the safety regulations for subcutaneous home self-administration of immunoglobulins as well as (2) guidelines for the prevention of anaphylaxis in patients receiving immunoglobulins (for example peanut).

免疫球蛋白替代疗法期间发生的过敏反应,尤其是过敏反应,较为罕见,但其病理生理学和分类仍不明确。最近的研究结果显示,使用市售免疫球蛋白进行皮肤试验有阳性结果,但受试免疫球蛋白的靶抗原和相关化合物尚未得到严格鉴定。
4例近期诊断为常见变异型免疫缺陷的成年患者符合标准的皮下免疫球蛋白替代治疗方案。他们既往无免疫球蛋白、血液或血液制品输注史。皮下免疫球蛋白输注部位出现水肿、融合性风团和红斑:典型的早期和晚期反应。各种被动转移的IgG和IgE抗体短暂升高导致了诸如I型过敏、抗Rh、同种血凝素和类风湿因子(RF)等活性体液反应的血清学检测出现误导性阳性结果。尽管临床表现非常罕见且严重,但回顾性分析显示患者血清中之前无同种血凝素、RF和IgE,但输注后呈阳性(IgE中位数 = 18 IU/ml,RF = 8 IU/ml)。在替代治疗第14天患者下乡时出现了I型过敏反应(喉头水肿、鼻结膜炎)。在第二位患者中,皮下注射免疫球蛋白5天后观察到过敏反应,且仅在患者食用花生时出现。因此,对一系列在最初皮下免疫球蛋白替代治疗中导致不良事件(AE)的市售制剂进行回顾性IgE浓度测定,结果为138至232 IU/ml(kU/l),即每克蛋白质690 - 2100 IU。特异性IgE范围广泛,从198(食物混合物)到2809 kUA/l(草混合物),但许多受试变应原特异性IgE为2级或3级(即0.71 - 17.5 kUA/l)。
该病例类似于被动皮肤过敏反应和普劳斯尼茨 - 屈斯特纳反应,但尚未描述这些经典现象的临床意义。这一观察结果表明,免疫球蛋白替代疗法期间的过敏反应可能由IgE或病理性IgG含量引起。在医疗专业人员使用和监测的静脉注射免疫球蛋白中曾偶尔报告过此类IgE的存在(34.5 - 105 IU/ml,即每克蛋白质862.5 - 1450 IU)。在临床实践中,不良事件的定义并不充分,因为各批次免疫球蛋白具有不同的特异性,因此,它们应归类为输血产品(而非生物等效物)。这种新方法意味着要建立(1)新的控制方法和策略,以确保引入皮下家庭自我注射免疫球蛋白的安全规定,以及(2)接受免疫球蛋白治疗患者(如对花生过敏者)预防过敏反应的指南。