Centre for Infectious Disease Epidemiology & Research, School of Public Health & Family Medicine, University of Cape Town, Cape Town, South Africa.
Division of Epidemiology and Biostatistics, School of Public Health & Family Medicine, University of Cape Town, Cape Town, South Africa.
J Int AIDS Soc. 2017 Sep 25;20(1):21902. doi: 10.7448/IAS.20.1.21902.
South Africa has the largest number of individuals living with HIV and the largest antiretroviral therapy (ART) programme worldwide. In September 2016, ART eligibility was extended to all 7.1 million HIV-positive South Africans. To ensure that further expansion of services does not compromise quality of care, long-term outcomes must be monitored. Few studies have reported long-term mortality in resource-constrained settings, where mortality ascertainment is challenging. Combining site records with data linked to the national vital registration system, sites in the International Epidemiology Databases to Evaluate AIDS Southern Africa collaboration can identify >95% of deaths in patients with civil identification numbers (IDs). This study used linked data to explore long-term mortality and viral suppression among adults starting ART in South Africa.
The study was a cohort analysis of routine data on adults with IDs starting ART 2004-2015 in five large ART cohorts. Mortality was estimated overall and by gender using the Kaplan-Meier estimator and Cox's proportional hazards regression. Standardized mortality ratios (SMRs) were calculated by dividing observed numbers of deaths by numbers expected if patients had been HIV-negative. Viral suppression in patients with viral loads (VLs) in their last year of follow-up was the secondary outcome.
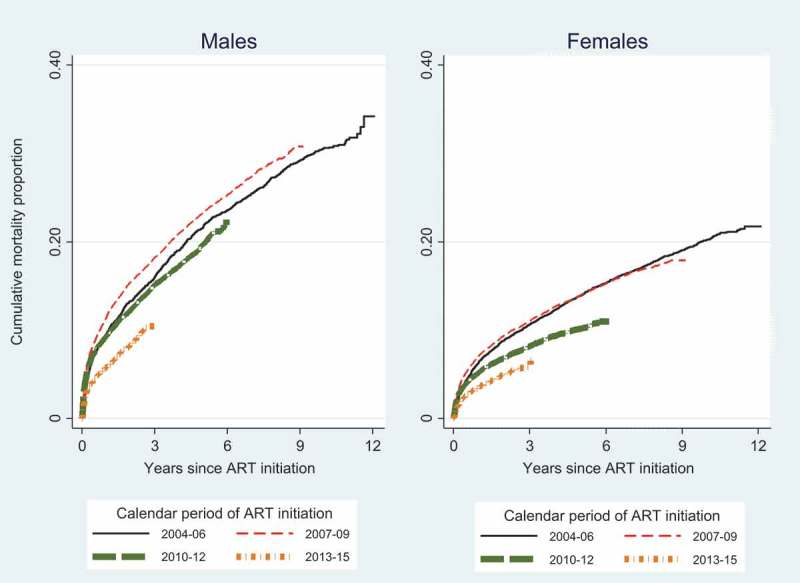
Among 72,812 adults followed for 350,376 person years (pyrs), the crude mortality rate was 3.08 (95% CI 3.02-3.14)/100 pyrs. Patients were predominantly female (67%) and the percentage of men initiating ART did not increase. Cumulative mortality 12 years after ART initiation was 23.9% (33.4% male and 19.4% female). Mortality peaked in patients enrolling in 2007-2009 and was higher in men than women at all durations. Observed mortality rates were higher than HIV-negative mortality, decreasing with duration. By 48 months, observed mortality was close to that in the HIV-negative population, and SMRs were similar for all baseline CD4 strata. Three-quarters of patients had VLs in their last year, and 86% of these were virally suppressed.
The South African ART programme has shown a remarkable ability to initiate and manage patients successfully over 12 years, despite rapid expansion. With further scale-up, testing and initiating men on ART must be a national priority.
南非拥有世界上数量最多的艾滋病毒感染者和最大的抗逆转录病毒治疗(ART)项目。2016 年 9 月,ART 的资格扩大到所有 710 万艾滋病毒阳性的南非人。为了确保进一步扩大服务不会影响护理质量,必须监测长期结果。在资源有限的环境中,死亡率确定具有挑战性,很少有研究报告长期死亡率。通过将站点记录与国家生命登记系统相关联的数据相结合,国际流行病学数据库评估艾滋病南部非洲合作组织的站点可以识别出具有公民身份识别号码(ID)的患者中超过 95%的死亡。本研究使用关联数据来探讨南非开始接受抗逆转录病毒治疗的成年人的长期死亡率和病毒抑制情况。
本研究是对 2004 年至 2015 年五个大型抗逆转录病毒治疗队列中 ID 号成人开始抗逆转录病毒治疗的常规数据进行的队列分析。使用 Kaplan-Meier 估计器和 Cox 比例风险回归整体和按性别估计死亡率。标准化死亡率比(SMR)是通过将观察到的死亡人数除以如果患者 HIV 阴性的预期死亡人数来计算的。在最后一年的随访中有病毒载量(VL)的患者的病毒抑制是次要结果。
在 72812 名随访 350376 人年(pyrs)的成年人中,粗死亡率为 3.08(95%CI 3.02-3.14)/100 pyrs。患者主要为女性(67%),开始接受抗逆转录病毒治疗的男性比例没有增加。抗逆转录病毒治疗开始后 12 年的累积死亡率为 23.9%(男性 33.4%,女性 19.4%)。死亡率在 2007-2009 年登记的患者中达到峰值,并且在所有时间段内男性死亡率均高于女性。观察到的死亡率高于 HIV 阴性死亡率,随着时间的推移而降低。在 48 个月时,观察到的死亡率接近 HIV 阴性人群,所有基线 CD4 分层的 SMR 相似。四分之三的患者在最后一年的 VLs 中,其中 86%的患者病毒得到抑制。
尽管快速扩张,南非的抗逆转录病毒治疗计划在 12 年内成功启动和管理患者方面表现出了非凡的能力。随着进一步扩大规模,检测和为男性提供抗逆转录病毒治疗必须成为国家优先事项。