Pranzatelli Michael R, Tate Elizabeth D, McGee Nathan R
National Pediatric Myoclonus Center, Neuroimmunology Laboratory, Orlando, FL, United States.
National Pediatric Neuroinflammation Organization, Inc., Orlando, FL, United States.
Front Neurol. 2017 Sep 11;8:468. doi: 10.3389/fneur.2017.00468. eCollection 2017.
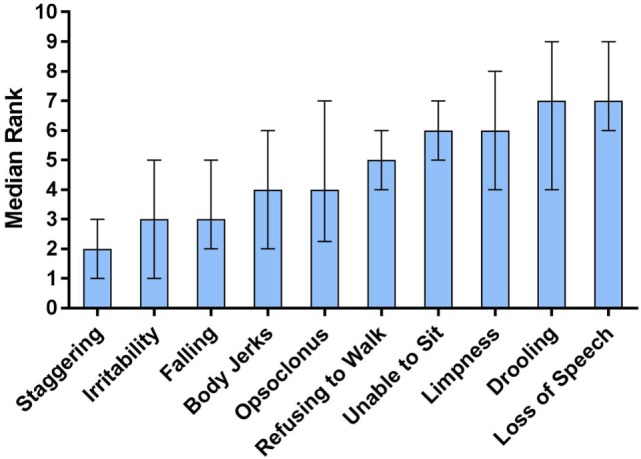
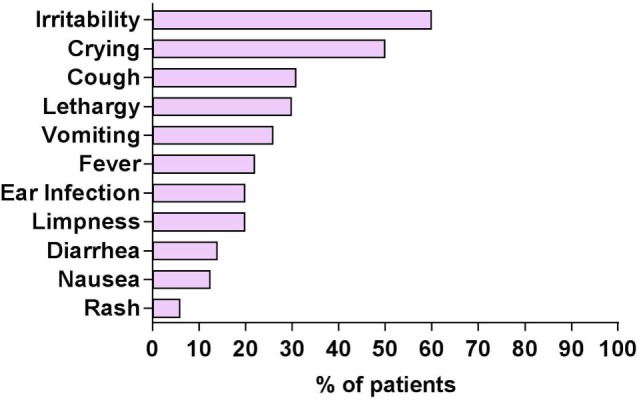
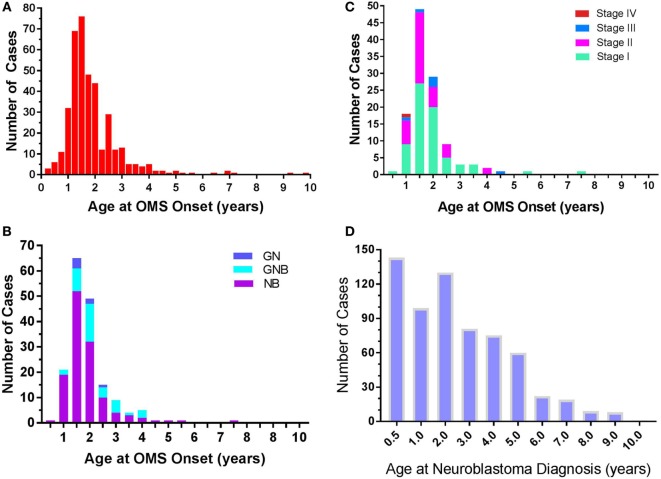
Pediatric-onset opsoclonus-myoclonus syndrome (OMS) is a devastating neuroinflammatory, often paraneoplastic, disorder. The objective was to characterize demographic, clinical, and immunologic aspects in the largest cohort reported to date. Cross-sectional data were collected on 389 children in an IRB-approved, observational study at the National Pediatric Myoclonus Center. Non-parametric statistical analysis was used. OMS manifested in major racial/ethnic groups, paralleling US population densities. Median onset age was 1.5 years (1.2-2 interquartile range), inclusive of infants (14%), toddlers (61%), and youngsters (25%). The higher female sex ratio of 1.2 was already evident in toddlers. Time to diagnosis was 1.2 months (0.7-3); to treatment, 1.4 months (0.4-4). Irritability/crying dominated prodromal symptomatology (60%); overt infections in <35%. Acute cerebellar ataxia was the most common misdiagnosis; staggering appeared earliest among 10 ranked neurological signs ( < 0.0001). Some untreated youngsters had no words (33%) or sentences (73%). Remote neuroblastic tumors were detected in 50%; resection was insufficient OMS treatment (58%). Age at tumor diagnosis related to tumor type ( = 0.004) and stage ( = 0.002). A novel observation was that paraneoplastic frequency varied with patient age-not a mere function of the frequency of neuroblastoma, which was lowest in the first 6 months of life, when that of neuroblastoma without OMS was highest. The cerebrospinal fluid (CSF) leukocyte count was minimally elevated in 14% (≤11/mm) with normal differential, and commercially screened serum autoantibodies were negative, but CSF oligoclonal bands (OCB) and B cells frequency were positive (58 and 93%). Analysis of patients presenting on immunotherapy revealed a shift in physician treatment practice patterns from monotherapy toward multi-agent immunotherapy ( < 0.001); the number of agents/sequences varied. In sum, a major clinical challenge is to increase OMS recognition, prevent initial misdiagnosis, and shorten time to diagnosis/treatment. The index of suspicion for an underlying tumor must remain high despite symptoms of infection. The disparity in onset age of neuroblastoma frequency with that of neuroblastoma with OMS warrants further studies of potential host/tumor factors. OMS neuroinflammation is best diagnosed by CSF OCB and B cells, not by routine CSF or commercial antibody studies.
儿童期起病的眼阵挛-肌阵挛综合征(OMS)是一种严重的神经炎症性疾病,通常为副肿瘤性疾病。目的是在迄今为止报告的最大队列中描述人口统计学、临床和免疫学方面的特征。在国家儿科肌阵挛中心一项经机构审查委员会批准的观察性研究中,收集了389名儿童的横断面数据。采用非参数统计分析。OMS在主要种族/族裔群体中均有表现,与美国人口密度情况相似。发病年龄中位数为1.5岁(四分位间距为1.2 - 2岁),包括婴儿(14%)、幼儿(61%)和儿童(25%)。在幼儿中,女性性别比为1.2,这一较高比例已很明显。诊断时间为1.2个月(0.7 - 3个月);开始治疗时间为1.4个月(0.4 - 4个月)。前驱症状中易激惹/哭闹最为常见(60%);明显感染的比例不到35%。急性小脑性共济失调是最常见的误诊疾病;蹒跚步态在10种排名靠前的神经系统体征中出现最早(P < 0.0001)。一些未经治疗的儿童不会说话(33%)或不会造句(73%)。50%的患者检测到既往神经母细胞瘤;肿瘤切除作为OMS的治疗并不充分(58%)。肿瘤诊断时的年龄与肿瘤类型(P = 0.004)和分期(P = 0.002)相关。一项新的观察结果是,副肿瘤性疾病的发生率随患者年龄而异——这不仅仅是神经母细胞瘤发生率的函数,神经母细胞瘤在生命的前6个月发生率最低,而无OMS的神经母细胞瘤发生率在此期间最高。14%的患者脑脊液(CSF)白细胞计数轻度升高(≤11/mm³),分类正常,商业筛查的血清自身抗体为阴性,但脑脊液寡克隆区带(OCB)和B细胞频率为阳性(分别为58%和93%)。对接受免疫治疗的患者分析显示,医生的治疗实践模式从单一疗法转向多药联合免疫治疗(P < 0.001);药物/疗程数量各不相同。总之,一个主要的临床挑战是提高对OMS的认识,防止最初的误诊,并缩短诊断/治疗时间。尽管有感染症状,但对潜在肿瘤的怀疑指数仍必须保持较高。神经母细胞瘤发生率与伴OMS的神经母细胞瘤发病年龄的差异值得对潜在的宿主/肿瘤因素进行进一步研究。OMS神经炎症最好通过脑脊液OCB和B细胞来诊断,而不是通过常规脑脊液或商业抗体检测。