Connolly Adam, Robson Matthew D, Schneider Jürgen, Burton Rebecca, Plank Gernot, Bishop Martin J
Department of Biomedical Engineering, Division of Imaging Sciences and Biomedical Engineering, King's College London, London, United Kingdom.
Division of Cardiovascular Medicine, University of Oxford, Oxford, United Kingdom.
Chaos. 2017 Sep;27(9):093913. doi: 10.1063/1.4999609.
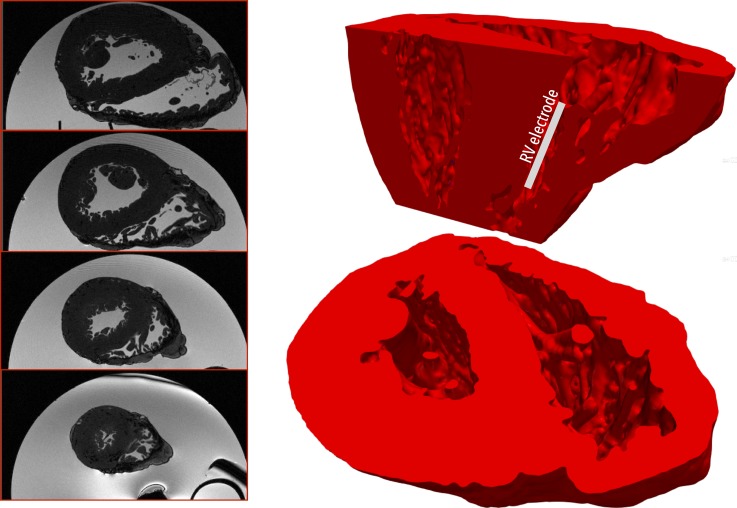
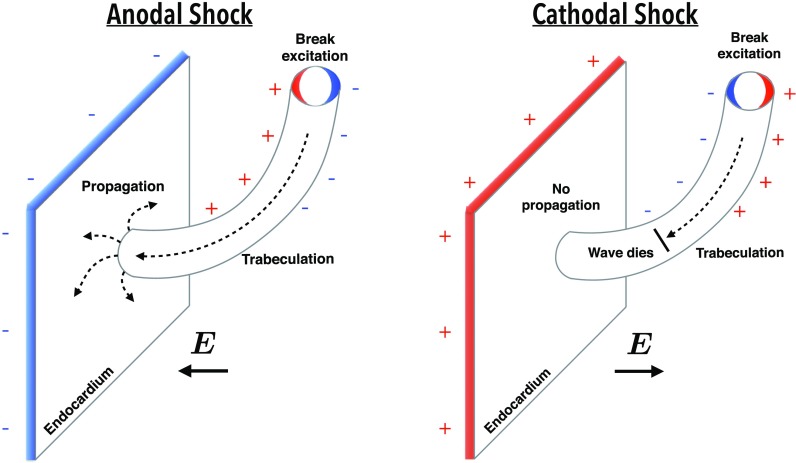
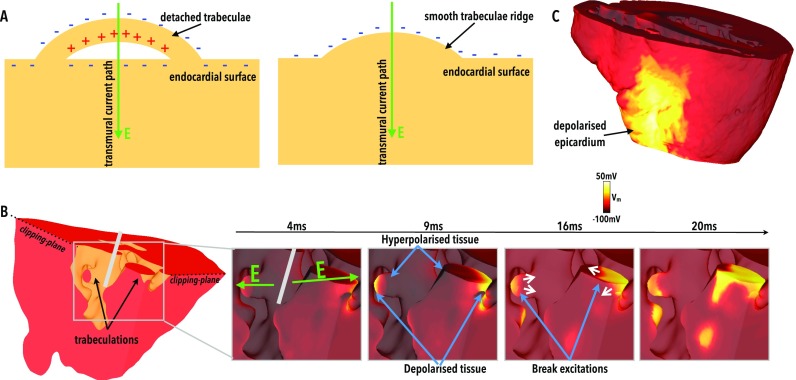
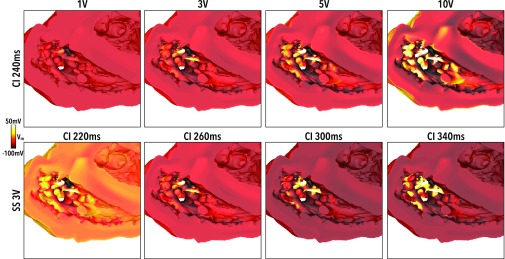
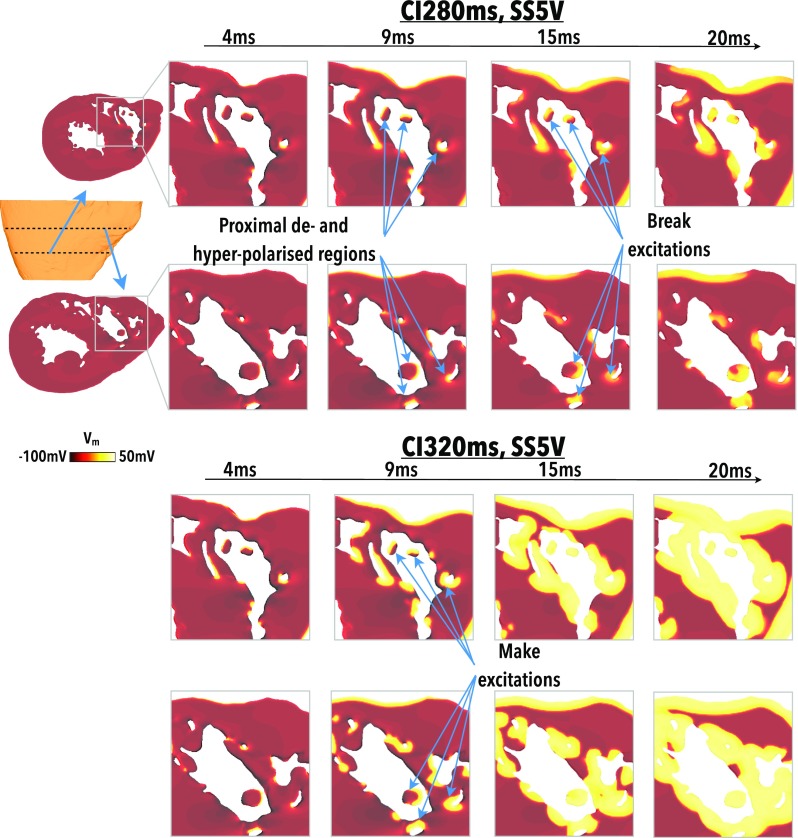
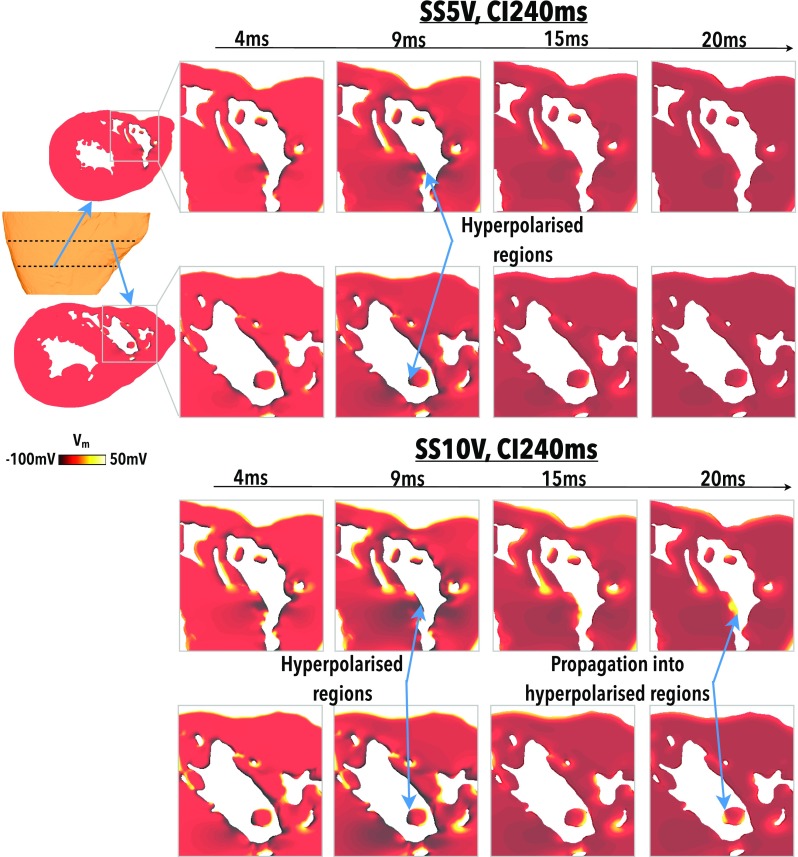
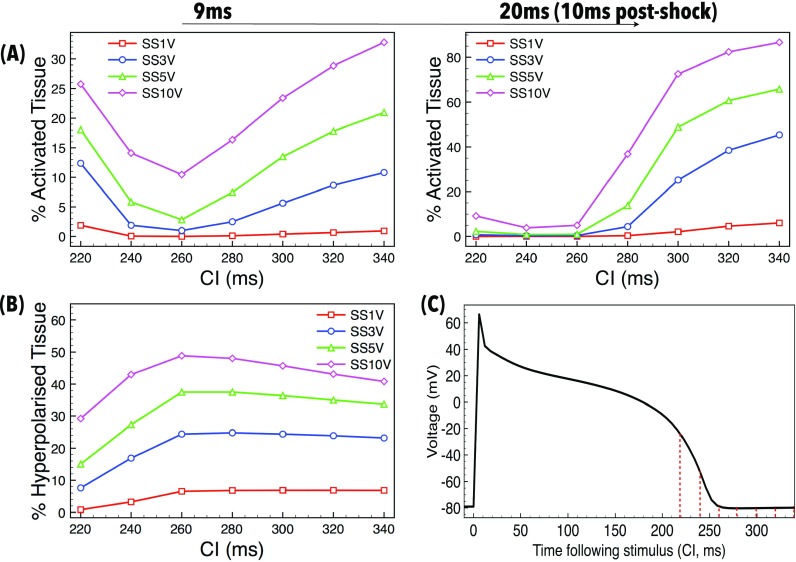
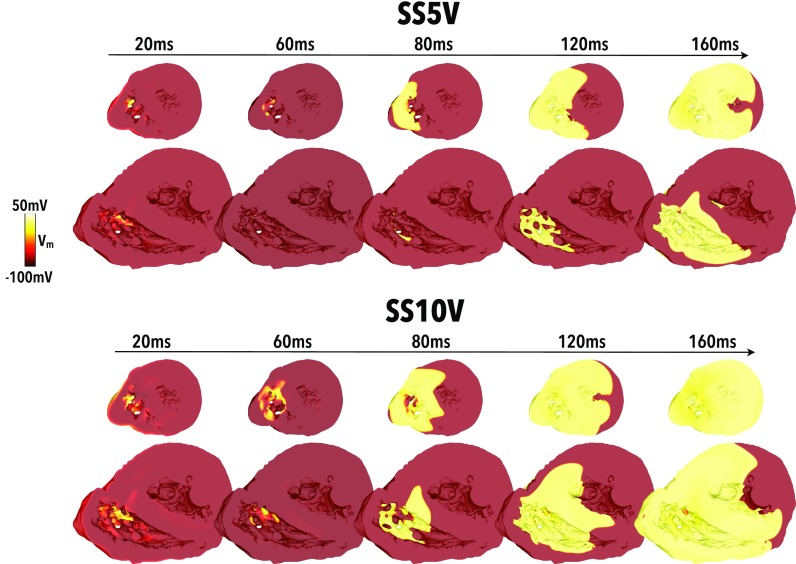
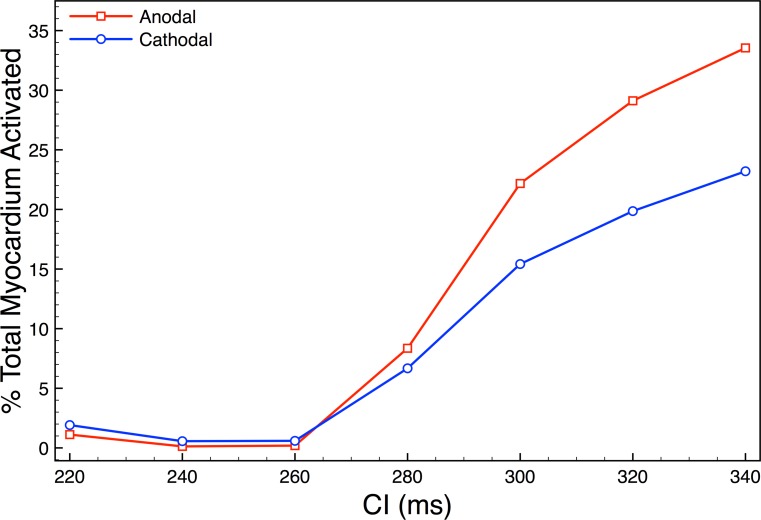
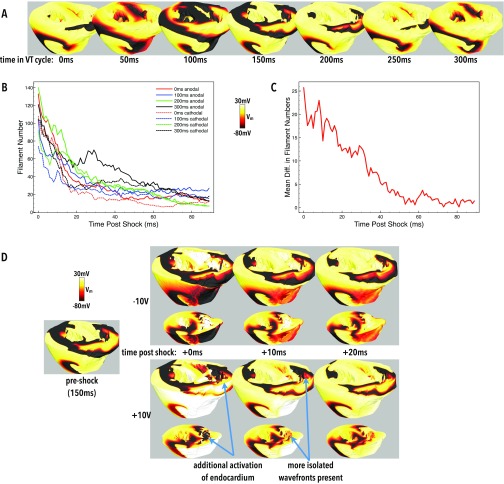
Novel low-energy defibrillation therapies are thought to be driven by virtual-electrodes (VEs), due to the interaction of applied monophasic electric shocks with fine-scale anatomical structures within the heart. Significant inter-species differences in the cardiac (micro)-anatomy exist, however, particularly with respect to the degree of endocardial trabeculations, which may underlie important differences in response to low-energy defibrillation protocols. Understanding the interaction of monophasic electric fields with the specific human micro-anatomy is therefore imperative in facilitating the translation and optimisation of these promising experimental therapies to the clinic. In this study, we sought to investigate how electric fields from implanted devices interact with the highly trabeculated human endocardial surface to better understand shock success in order to help optimise future clinical protocols. A bi-ventricular human computational model was constructed from high resolution (350 μm) ex-vivo MR data, including anatomically accurate endocardial structures. Monophasic shocks were applied between a basal right ventricular catheter and an exterior ground. Shocks of varying strengths were applied with both anodal [positive right ventricle (RV) electrode] and cathodal (negative RV electrode) polarities at different states of tissue refractoriness and during induced arrhythmias. Anodal shocks induced isolated positive VEs at the distal side of "detached" trabeculations, which rapidly spread into hyperpolarised tissue on the surrounding endocardial surfaces following the shock. Anodal shocks thus depolarised more tissue 10 ms after the shock than cathodal shocks where the propagation of activation from VEs induced on the proximal side of "detached" trabeculations was prevented due to refractory endocardium. Anodal shocks increased arrhythmia complexity more than cathodal shocks during failed anti-arrhythmia shocks. In conclusion, multiple detached trabeculations in the human ventricle interact with anodal stimuli to induce multiple secondary sources from VEs, facilitating more rapid shock-induced ventricular excitation compared to cathodal shocks. Such a mechanism may help explain inter-species differences in response to shocks and help to develop novel defibrillation strategies.
新型低能量除颤疗法被认为是由虚拟电极(VEs)驱动的,这是由于施加的单相电击与心脏内精细尺度的解剖结构相互作用所致。然而,心脏(微观)解剖结构存在显著的种间差异,特别是在心内膜小梁化程度方面,这可能是对低能量除颤方案反应存在重要差异的基础。因此,了解单相电场与特定人体微观解剖结构的相互作用对于推动这些有前景的实验性疗法转化并优化至临床至关重要。在本研究中,我们试图研究植入设备产生的电场如何与高度小梁化的人体心内膜表面相互作用,以更好地理解电击成功的机制,从而帮助优化未来的临床方案。利用高分辨率(350μm)的离体磁共振数据构建了双心室人体计算模型,包括解剖结构精确的心内膜结构。在右心室基部导管和外部接地之间施加单相电击。在不同的组织不应期状态和诱发心律失常期间,分别以阳极[右心室(RV)电极正极]和阴极(右心室电极负极)极性施加不同强度的电击。阳极电击在“分离”小梁的远端诱导出孤立的正性虚拟电极,电击后这些虚拟电极迅速扩散到周围心内膜表面的超极化组织中。因此,与阴极电击相比,阳极电击在电击后10毫秒使更多组织去极化,因为在“分离”小梁近端诱导的虚拟电极的激活传播由于不应期心内膜而受到阻碍。在抗心律失常电击失败期间,阳极电击比阴极电击更能增加心律失常的复杂性。总之,人体心室中的多个分离小梁与阳极刺激相互作用,从虚拟电极诱导出多个次级源,与阴极电击相比,促进了电击诱导的心室兴奋更快发生。这种机制可能有助于解释种间对电击反应的差异,并有助于开发新的除颤策略。