Grabar Sophie, Selinger-Leneman Hana, Abgrall Sophie, Pialoux Gilles, Weiss Laurence, Costagliola Dominique
Sorbonne Universités, INSERM, UPMC Univ Paris 06, Institut Pierre Louis d'épidémiologie et de Santé Publique (IPLESP UMRS 1136), F75013, Paris, France.
Assistance Publique Hôpitaux de Paris (AP-HP), Groupe hospitalier Cochin Broca Hôtel-Dieu, Unité de Biostatistique et d'épidémiologie, Paris, France.
PLoS One. 2017 Oct 2;12(10):e0184441. doi: 10.1371/journal.pone.0184441. eCollection 2017.
We studied the frequency and risk factors for loss of long-term non-progressor (LTNP) and HIV controller (HIC) status among patients identified as such in 2005 in the French Hospital Database on HIV (FHDH-ANRS CO4).
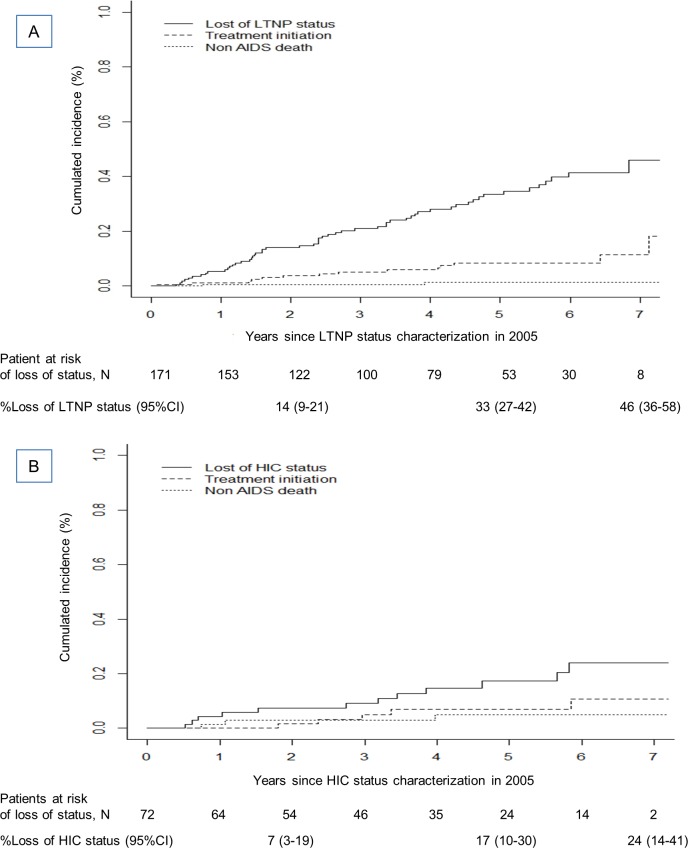
We selected patients who were treatment-naïve and asymptomatic in 2005 (baseline). Those with ≥8 years of known HIV infection and a CD4 cell nadir ≥500/mm3 were classified as LTNP and those with ≥10 years of known HIV infection and 90% of plasma viral load (VL) values ≤500 copies/ml in the absence of cART as HIC. cART initiation without loss of status and death from non AIDS-defining causes were considered as competing events.
After 5 years of follow-up, 33% (95%CI; 27-42) of 171 LTNP patients and 17% (95%CI; 10-30) of 72 HIC patients had lost their status. In multivariable analyses, loss of LTNP status was associated with lower baseline CD4 cell counts and CD4/CD8 ratios. Only VL was significantly associated with loss of HIC status after adjustment for the baseline CD4 cell count, the CD4/CD8 ratio, and concomitant LTNP status. The hazard ratio for loss of HIC status was 5.5 (95%CI, 1.5-20.1) for baseline VL 50-500 vs ≤50 cp/mL, after adjustment for the baseline CD4 cell count.
One-third of LTNP and one-fifth of HIC patients lost their status after 5 years of follow-up, raising questions as to the possible benefits and timing of ART initiation in these populations.
我们在法国医院HIV数据库(FHDH-ANRS CO4)中研究了2005年被确定为长期无进展者(LTNP)和HIV控制者(HIC)的患者失去该状态的频率及危险因素。
我们选取了2005年(基线)未经治疗且无症状的患者。已知感染HIV时间≥8年且CD4细胞最低点≥500/mm³的患者被分类为LTNP,已知感染HIV时间≥10年且在未接受抗逆转录病毒治疗(cART)时血浆病毒载量(VL)值90%≤500拷贝/ml的患者被分类为HIC。未失去状态而开始cART以及非艾滋病定义原因导致的死亡被视为竞争事件。
经过5年随访,171例LTNP患者中有33%(95%CI:27 - 42)、72例HIC患者中有17%(95%CI:10 - 30)失去了他们的状态。在多变量分析中,LTNP状态的丧失与较低的基线CD4细胞计数和CD4/CD8比值相关。在对基线CD4细胞计数、CD4/CD8比值及伴随的LTNP状态进行调整后,仅VL与HIC状态的丧失显著相关。在对基线CD4细胞计数进行调整后,基线VL为50 - 500 vs≤50拷贝/ml时,HIC状态丧失的风险比为5.5(95%CI,1.5 - 20.1)。
经过5年随访,三分之一的LTNP患者和五分之一的HIC患者失去了他们的状态,这引发了关于在这些人群中开始抗逆转录病毒治疗的可能益处和时机的问题。