Department of Hematology and Oncology, Graduate School of Medicine, Kyoto University, Japan.
Laboratory of Clinical Immunology and Microbiology, National Institute of Allergy and Infectious Diseases, National Institutes of Health, Bethesda, MD, USA.
Haematologica. 2018 Jan;103(1):163-171. doi: 10.3324/haematol.2017.174615. Epub 2017 Sep 29.
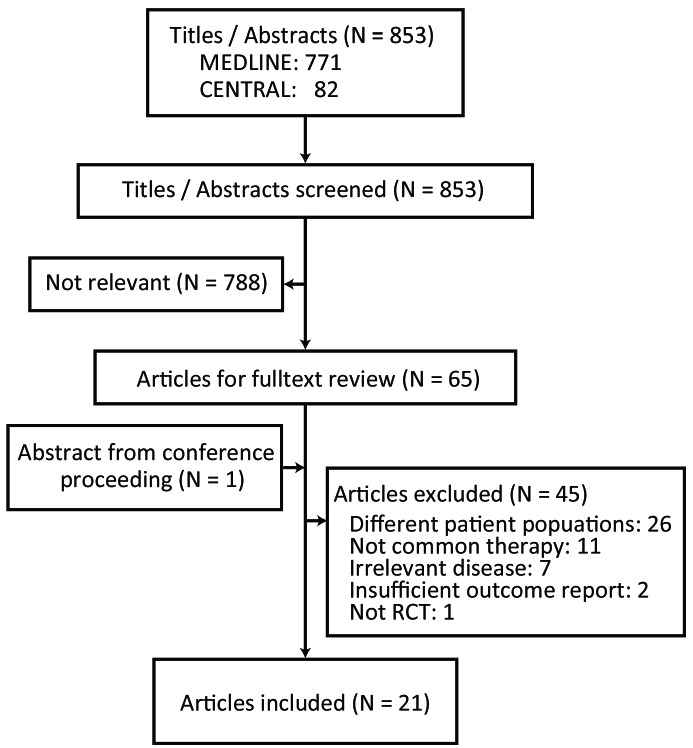
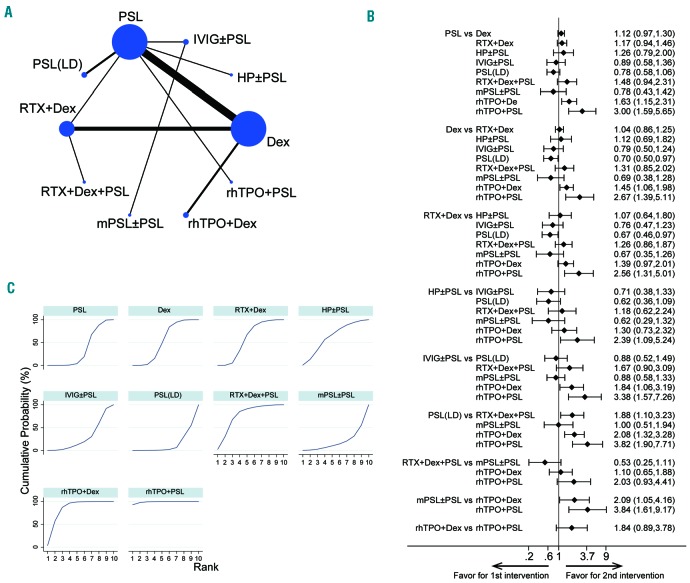
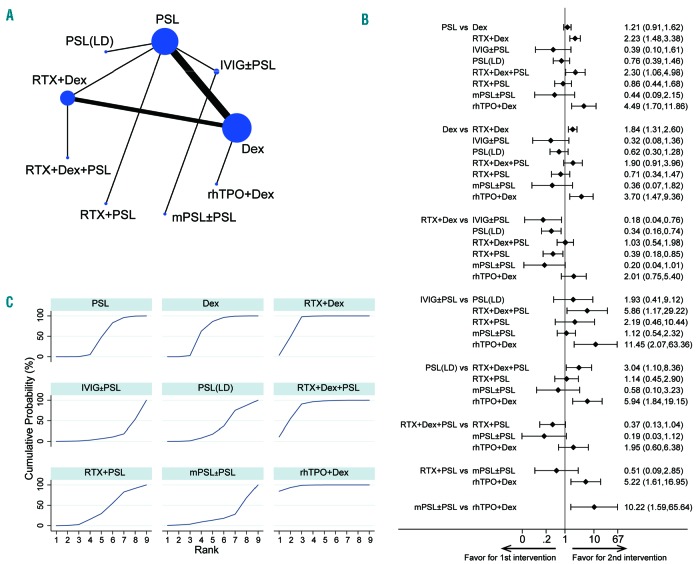
Corticosteroids such as prednisolone and dexamethasone have been established as up-front therapy for the treatment of newly diagnosed immune thrombocytopenia. Recent studies have indicated that other treatments such as rituximab or thrombopoietin receptor agonist can also be effective choices. We performed a systematic review and network meta-analysis to establish a clinically meaningful hierarchy of efficacy and safety of treatments for newly diagnosed primary immune thrombocytopenia in adults. Randomized controlled trials evaluating medical treatments for newly diagnosed immune thrombocytopenia were included. Reviewers independently extracted data and assessed the risk of bias. The main outcome was the sustained response (platelet count >30×10/L for 3-6 months after completion of treatments), while overall response (platelet count >30×10/L for 2-4 weeks after initiation of the up-front treatment) and therapy-related adverse events were the secondary endpoints. A total of 21 randomized controlled trials (1898 patients) were included in this study. Our main findings were a significantly better sustained response in the recombinant human thrombopoietin+dexamethasone and rituximab+dexamethasone arms compared to those of conventional therapies (prednisolone and dexamethasone monotherapy). Moreover, recombinant human thrombopoietin+dexamethasone and +prednisolone improved early overall response compared to prednisolone, dexamethasone, and rituximab-containing regimens. Therapy-related adverse events showed similar profiles and were tolerable in all treatment arms. Regimens containing recombinant human thrombopoietin agonist may be beneficial up-front therapies in addition to the conventional corticosteroid monotherapies. Future head-to-head trials including these regimens and rituximab-containing treatments are necessary in order to overcome the limitations of the small number in our study and determine the most suitable initial therapies for newly diagnosed immune thrombocytopenia.
皮质类固醇,如泼尼松龙和地塞米松,已被确立为治疗新诊断免疫性血小板减少症的一线治疗方法。最近的研究表明,其他治疗方法,如利妥昔单抗或血小板生成素受体激动剂,也可以是有效的选择。我们进行了一项系统评价和网络荟萃分析,以确定治疗成人新诊断原发性免疫性血小板减少症的疗效和安全性的临床有意义的层次结构。纳入了评估新诊断免疫性血小板减少症的医学治疗的随机对照试验。审查员独立提取数据并评估偏倚风险。主要结局是持续反应(治疗完成后 3-6 个月血小板计数> 30×10/L),而总体反应(起始治疗后 2-4 周血小板计数> 30×10/L)和治疗相关不良事件是次要终点。这项研究共纳入 21 项随机对照试验(1898 例患者)。我们的主要发现是与常规治疗(泼尼松龙和地塞米松单药治疗)相比,重组人血小板生成素+地塞米松和利妥昔单抗+地塞米松组的持续反应显著更好。此外,与泼尼松龙、地塞米松和含利妥昔单抗的方案相比,重组人血小板生成素+地塞米松和+泼尼松龙改善了早期总体反应。治疗相关不良事件在所有治疗组中具有相似的特征且可耐受。除了常规皮质类固醇单药治疗外,含有重组人血小板生成素激动剂的方案可能是有益的一线治疗方法。为了克服我们研究中数量较少的局限性,并确定最适合新诊断免疫性血小板减少症的初始治疗方法,有必要进行包括这些方案和含利妥昔单抗治疗的头对头试验。