Oxford Centre for Clinical Magnetic Resonance Research, University of Oxford, Oxford, UK.
Int J Obes (Lond). 2018 Mar;42(3):441-447. doi: 10.1038/ijo.2017.239. Epub 2017 Oct 4.
Obesity causes diastolic dysfunction, and is one of the leading causes of heart failure with preserved ejection fraction. Myocardial relaxation is determined by both active metabolic processes such as impaired energetic status and steatosis, as well as intrinsic myocardial remodelling. However, the relative contribution of each to diastolic dysfunction in obesity is currently unknown.
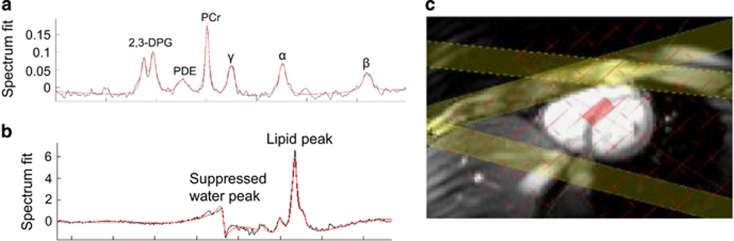
Eighty adult subjects (48 male) with no cardiovascular risk factors across a wide range of body mass indices (18.4-53.0 kg m) underwent magnetic resonance imaging for abdominal visceral fat, left ventricular geometry (LV mass:volume ratio) and diastolic function (peak diastolic strain rate), and magnetic resonance spectroscopy for PCr/ATP and myocardial triglyceride content.
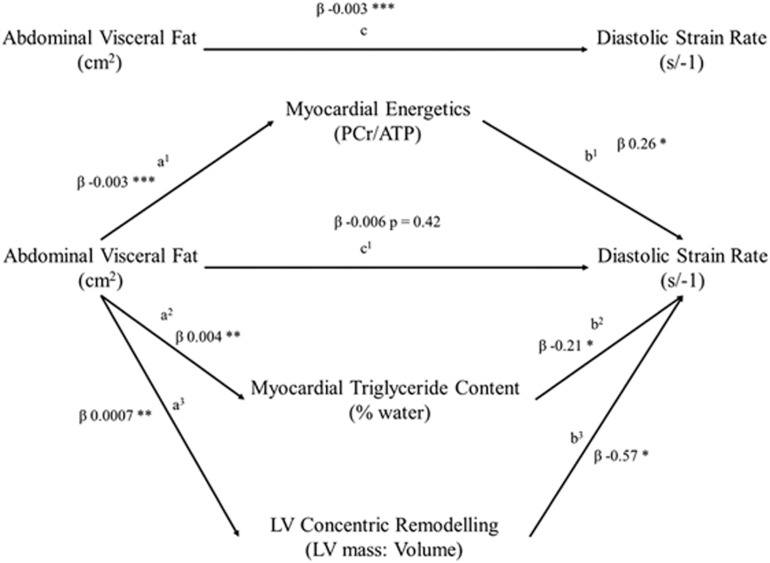
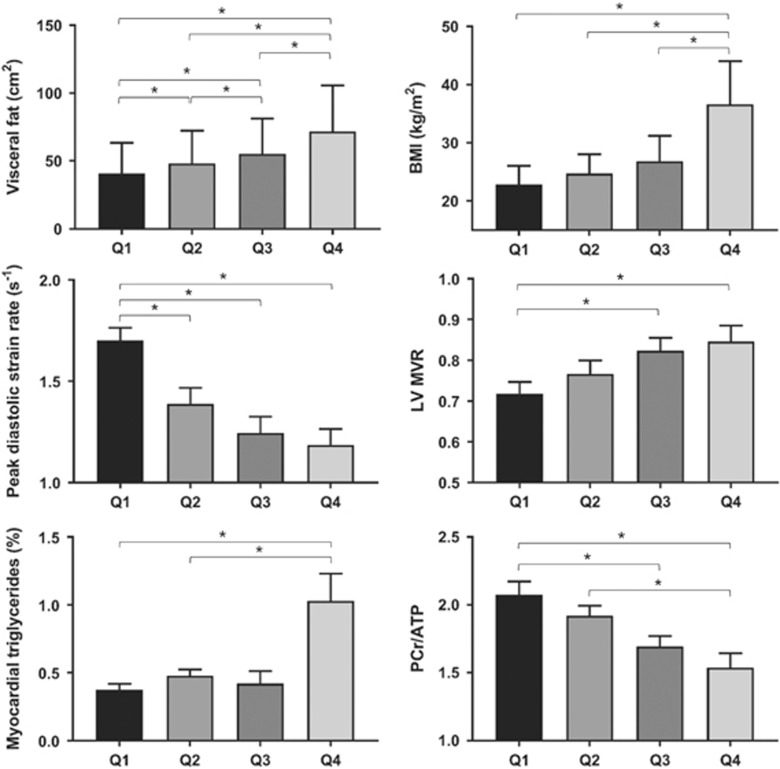
Increasing visceral obesity was related to diastolic dysfunction (peak diastolic strain rate, r=-0.46, P=0.001). Myocardial triglyceride content (β=-0.2, P=0.008), PCr/ATP (β=-0.22, P=0.04) and LV mass:volume ratio (β=-0.61, P=0.04) all independently predicted peak diastolic strain rate (model R 0.36, P<0.001). Moderated multiple regression confirmed the full mediating roles of PCr/ATP, myocardial triglyceride content and LV mass:volume ratio in the relationship between visceral fat and peak diastolic strain rate. Of the negative effect of visceral fat on diastolic function, 40% was explained by increased myocardial triglycerides, 39% by reduced PCr/ATP and 21% by LV concentric remodelling.
Myocardial energetics and steatosis are more important in determining LV diastolic function than concentric hypertrophy, accounting for more of the negative effect of obesity on diastolic function than LV geometric remodelling. Targeting these metabolic processes is an attractive strategy to treat diastolic dysfunction in obesity.
肥胖会导致舒张功能障碍,是射血分数保留型心力衰竭的主要病因之一。心肌舒张由代谢活性过程决定,如能量状态受损和脂肪变性,也由内在的心肌重塑决定。然而,肥胖导致舒张功能障碍时,每种因素的相对贡献尚不清楚。
80 名成年受试者(48 名男性),年龄在 20 岁至 79 岁之间,无心血管危险因素,体质量指数(BMI)范围为 18.4-53.0kg/m2,接受腹部内脏脂肪、左心室几何形状(左心室质量/容积比)和舒张功能(舒张末期峰值应变率)的磁共振成像,以及心肌三酰甘油含量和磷肌酸/ATP 的磁共振波谱检查。
随着内脏肥胖程度的增加,舒张功能障碍(舒张末期峰值应变率)也随之增加(r=-0.46,P=0.001)。心肌三酰甘油含量(β=-0.2,P=0.008)、磷肌酸/ATP(β=-0.22,P=0.04)和左心室质量/容积比(β=-0.61,P=0.04)均独立预测舒张末期峰值应变率(模型 R 为 0.36,P<0.001)。中介效应检验证实,磷肌酸/ATP、心肌三酰甘油含量和左心室质量/容积比在腹型肥胖与舒张末期峰值应变率之间的关系中具有完全的中介作用。腹型肥胖对舒张功能的负面影响中,有 40%是由心肌三酰甘油增加引起的,39%是由磷肌酸/ATP 减少引起的,21%是由左心室向心性重构引起的。
与向心性肥厚相比,心肌能量代谢和脂肪变性在决定左心室舒张功能方面更为重要,肥胖对舒张功能的负面影响中,由心肌代谢异常引起的部分多于由左心室几何重构引起的部分。针对这些代谢过程是治疗肥胖性舒张功能障碍的一种有吸引力的策略。