Rodrigo Emilio, Pich Sara, Subirana Isaac, Fernandez-Fresnedo Gema, Barreda Paloma, Ferrer-Costa Carles, M de Francisco Ángel Luis, Salas Eduardo, Elosua Roberto, Arias Manuel
Nephrology Service, University Hospital Marques de Valdecilla, Santander, Spain.
Instituto de Investigación Marqués de Valdecilla (IDIVAL), Santander, Spain.
Clin Kidney J. 2017 Oct;10(5):672-678. doi: 10.1093/ckj/sfx039. Epub 2017 Jun 22.
Coronary heart disease (CHD) is the primary cause of death in individuals with chronic kidney disease (CKD), but current equations for assessing coronary risk have low accuracy in this group. We have reported that the addition of a genetic risk score (GRS) to the Framingham risk function improved its predictive capacity in the general population. The aims of this study were to evaluate the association between this GRS and coronary events in the CKD population and to determine whether the addition of the GRS to coronary risk prediction functions improves the estimation of coronary risk at the earliest possible stages of kidney disease.
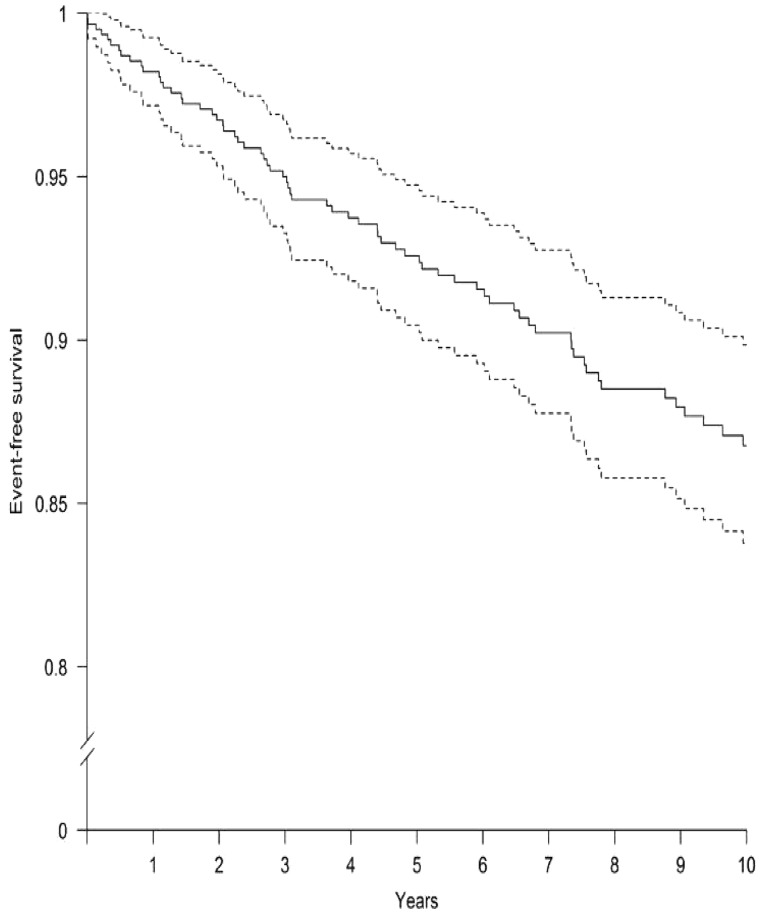
A total of 632 CKD patients, aged 35-74 years, who had Stage 4-5 CKD, were on dialysis, had a functioning renal transplant or had returned to dialysis after transplant failure were included and followed up for a mean of 9.3 years. The transitions between disease states and the development of coronary events were registered. The increase in predictive ability that was obtained by including the GRS was measured as the improvement in the C-statistic and as the net reclassification index.
The GRS was independently associated with the risk of CHD (hazards ratio 1.34; 95% confidence interval 1.04-1.71; P = 0.022), especially in Stages 4 and 5 CKD, and kidney transplant patients. A coronary risk prediction function that incorporated chronic kidney disease (CKD) disease state, age, sex and the GRS had significantly greater predictive capacity (AUC 70.1, P = 0.01) and showed good reclassification (net reclassification improvement 28.6).
This new function, combining genetic and clinical data, identifies CKD patients with a high risk of coronary events more accurately, allowing us to prevent such events more effectively.
冠心病(CHD)是慢性肾脏病(CKD)患者的主要死因,但目前用于评估冠心病风险的公式在该群体中的准确性较低。我们曾报道,在弗雷明汉风险函数中加入遗传风险评分(GRS)可提高其在一般人群中的预测能力。本研究的目的是评估该GRS与CKD人群冠心病事件之间的关联,并确定在冠心病风险预测函数中加入GRS是否能在肾病的最早阶段改善冠心病风险的估计。
共纳入632例年龄在35 - 74岁之间、患有4 - 5期CKD、正在接受透析、接受了功能性肾移植或移植失败后恢复透析的CKD患者,并对其进行了平均9.3年的随访。记录疾病状态之间的转变以及冠心病事件的发生情况。通过纳入GRS获得的预测能力的提高以C统计量的改善和净重新分类指数来衡量。
GRS与冠心病风险独立相关(风险比1.34;95%置信区间1.04 - 1.71;P = 0.022),尤其是在4期和5期CKD患者以及肾移植患者中。纳入慢性肾脏病(CKD)疾病状态、年龄、性别和GRS的冠心病风险预测函数具有显著更高的预测能力(AUC 70.1,P = 0.01),并显示出良好的重新分类(净重新分类改善28.6)。
这种结合遗传和临床数据的新函数能更准确地识别具有高冠心病事件风险的CKD患者,使我们能够更有效地预防此类事件。