Kute Vivek B, Patel Himanshu V, Shah Pankaj R, Modi Pranjal R, Shah Veena R, Rizvi Sayyed J, Pal Bipin C, Shah Priya S, Varyani Umesh T, Wakhare Pavan S, Shinde Saiprasad G, Ghodela Vijay A, Trivedi Varsha B, Patel Minaxi H, Trivedi Hargovind L
Department of Nephrology and Transplantation, Institute of Kidney Diseases and Research Center, Dr HL Trivedi Institute of Transplantation Sciences (IKDRC-ITS), Ahmedabad, India.
Department of Urology and Transplantation, IKDRC-ITS, Ahmedabad, India.
Clin Kidney J. 2017 Oct;10(5):709-714. doi: 10.1093/ckj/sfx032. Epub 2017 May 8.
To ascertain the validity of kidney paired donations (KPDs) as an alternative strategy for increasing living donor kidney transplantations (LDKTs) in an LDKT-dominated transplant programme since directed kidney transplantation, ABO-incompatible or crossmatch-positive pairs are not feasible due to costs and infectious complications.
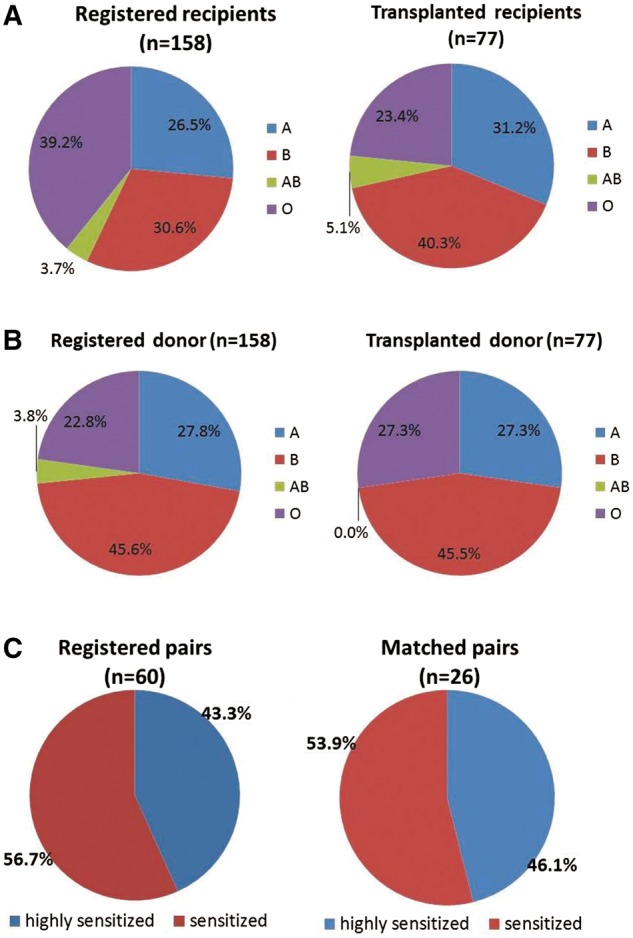
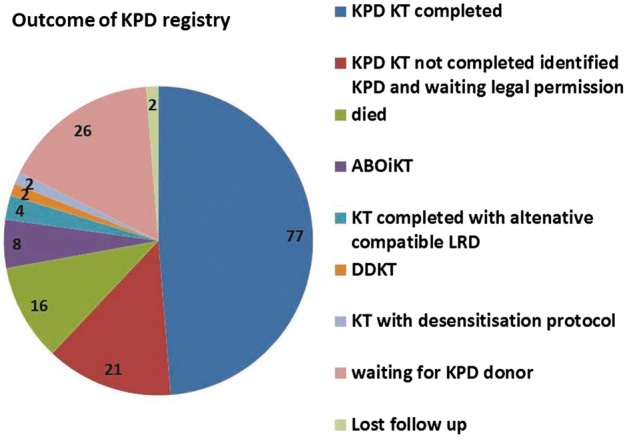
This was a prospective single-centre study of 77 KPD transplantations (25 two-way, 7 three-way and 1 six-way exchange) from 1 January 2015 to 1 January 2016 of 158 registered donor recipient pairs. During this period, a total of 380 kidney transplantations [71 deceased donor kidney transplantations (DDKTs), 309 LDKTs] were performed. The reasons for opting for KPD were ABO incompatibility ( = 45), sensitization ( = 26) and better matching ( = 6).
KPD matching was facilitated in 62% ( = 98) of transplants. In all, 48.7% ( = 77) of the transplants were completed in 2015, whereas 13.3% ( = 21) of the matched patients were to undergo transplant surgery in early 2016 after getting legal permission. The waiting time for KPD was shorter compared with DDKT. The death-censored graft survival and patient survival were 98.7% ( = 76) and 93.5% ( = 72), respectively. In all, 14.2% ( = 11) of patients had acute rejection. Match rates among sensitized ( = 60) and O group patients ( = 62) were 58.3% ( = 35) and 41.9% ( = 26), respectively. Of these, 43.3% ( = 26) and 29% ( = 18) of transplants were completed and 15% ( = 9) and 12.9% ( = 8), respectively, are waiting for legal permission.
LDKT increased by 25% in 1 year in our single-centre KPD programme. Our key to success was the formation of a KPD registry, awareness and active counselling programs and developing a dedicated team.
自从开展定向肾移植以来,由于成本和感染并发症问题,ABO血型不相容或交叉配型阳性的肾移植对在以活体供肾肾移植(LDKT)为主的移植项目中作为增加活体供肾移植数量的替代策略的有效性尚待确定。
这是一项前瞻性单中心研究,对2015年1月1日至2016年1月1日期间158对登记的供受者对中的77例肾移植配对捐赠(KPD)移植(25例双向、7例三向和1例六向交换)进行研究。在此期间,共进行了380例肾移植[71例尸体供肾肾移植(DDKT),309例LDKT]。选择KPD的原因是ABO血型不相容(n = 45)、致敏(n = 26)和更好的配型(n = 6)。
62%(n = 98)的移植手术实现了KPD配型。总共48.7%(n = 77)的移植手术在2015年完成,而13.3%(n = 21)的配型成功患者在获得法律许可后将于2016年初接受移植手术。KPD的等待时间比DDKT短。死亡截尾的移植物存活率和患者存活率分别为98.7%(n = 76)和93.5%(n = 72)。总共14.2%(n = 11)的患者发生了急性排斥反应。致敏患者(n = 60)和O型血患者(n = 62)的配型成功率分别为58.3%(n = 35)和41.9%(n = 26)。其中,43.3%(n = 26)和29%(n = 18)的移植手术已完成,分别有15%(n = 9)和12.9%(n = 8)的患者在等待法律许可。
在我们的单中心KPD项目中,1年内LDKT数量增加了25%。我们成功的关键是建立KPD登记系统、开展宣传和积极的咨询项目以及组建专业团队。