Liu Caojie, Lv Qingguo, Chen Xinlei, Ni Guangcheng, Hu Liru, Tong Nanwei, Zhang Yuwei
West China Hospital, Sichuan University, Chengdu, China.
Department of Endocrinology and Metabolism, West China Hospital of Sichuan University, Chengdu, China.
Endocr Connect. 2017 Nov;6(8):830-838. doi: 10.1530/EC-17-0232. Epub 2017 Oct 6.
Preoperative preparation for adrenalectomy for pheochromocytomas and paragangliomas (PPGL) is universally recognized as necessary, while the optimal strategy remains controversial. Our aims were to increase intraoperative hemodynamic stability, expedite postoperative recovery, decrease side effects and reduce costs for patients with PPGL undergoing adrenalectomy.
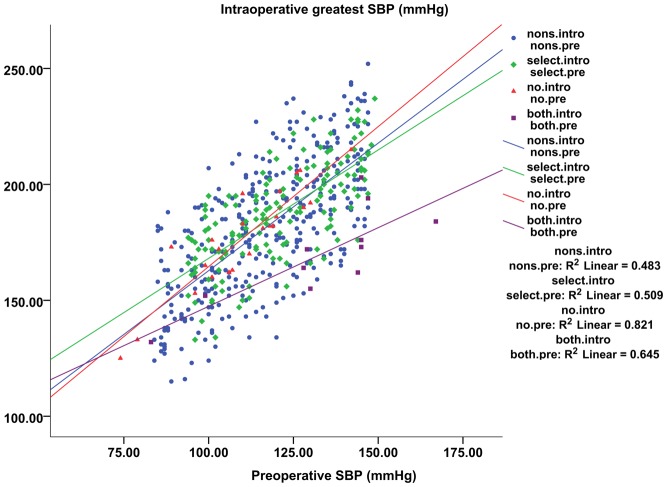
We identified 526 patients undergoing open adrenalectomy for PPGL in the West China Hospital of Sichuan University between May, 2007 and December, 2016. 149 patients received preoperative selective α-blockade with phenoxybenzamine, and 377 patients received non-selective α-blockade with prazosin, doxazosin or terazosin. There were no statistical differences between groups regarding preoperative patient and tumor characteristics. Operations were planned once hypertensive patients were well-controlled with blood pressure ≤130/85 mmHg. Intraoperatively, all patients received arterial blood pressure monitoring, and indwelling urinary catheters to record urine output. We recorded intraoperative hemodynamics, status in the postanesthesia or intensive care unit, postoperative recovery and complications.
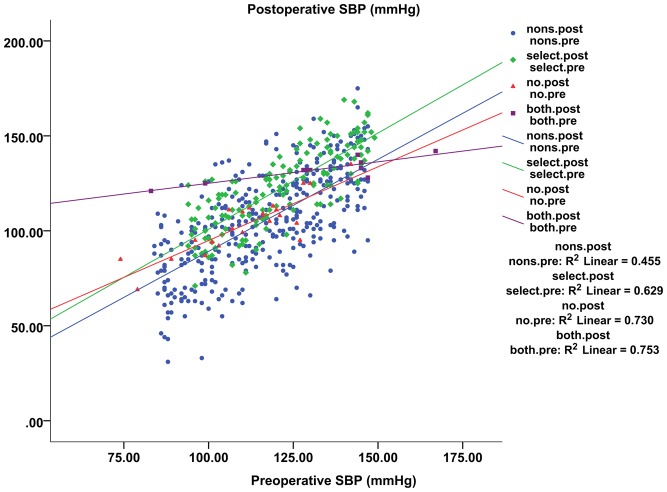
Patients in the non-selective group showed a more significant decline in postoperative systolic blood pressure than the selective group ( = 0.041). Also, patients in the non-selective group appeared to receive a long-term anti-hypertensive effect, especially for diastolic blood pressure ( = 0.037), which was a novel finding, based on the current literature.
Our results confirmed that non-selective α-blockade produced a more significant anti-hypertensive effect than selective α-blockade. However, we found no significant difference in intraoperative hemodynamic instability, postoperative recovery and postoperative complications between groups.
嗜铬细胞瘤和副神经节瘤(PPGL)肾上腺切除术的术前准备被普遍认为是必要的,但其最佳策略仍存在争议。我们的目的是提高PPGL患者肾上腺切除术术中的血流动力学稳定性,加快术后恢复,减少副作用并降低成本。
我们确定了2007年5月至2016年12月在四川大学华西医院接受开放性PPGL肾上腺切除术的526例患者。149例患者接受苯苄胺术前选择性α受体阻滞,377例患者接受哌唑嗪、多沙唑嗪或特拉唑嗪非选择性α受体阻滞。两组患者术前的患者和肿瘤特征无统计学差异。一旦高血压患者血压控制在≤130/85 mmHg,便计划进行手术。术中,所有患者均接受动脉血压监测,并留置导尿管以记录尿量。我们记录了术中血流动力学、麻醉后或重症监护病房的情况、术后恢复情况及并发症。
非选择性组患者术后收缩压下降幅度比选择性组更显著(=0.041)。此外,非选择性组患者似乎获得了长期降压效果,尤其是舒张压(=0.037),基于当前文献,这是一个新发现。
我们的结果证实,非选择性α受体阻滞比选择性α受体阻滞产生更显著的降压效果。然而,我们发现两组在术中血流动力学不稳定、术后恢复及术后并发症方面无显著差异。