Oguttu David W, Okullo A, Bwire G, Nsubuga P, Ario A R
Uganda Public Health Fellowship Program - Field Epidemiology Track, P.O. Box 7272, Kampala, Uganda.
Ministry of Health, Kampala, Uganda.
Infect Dis Poverty. 2017 Oct 10;6(1):146. doi: 10.1186/s40249-017-0359-2.
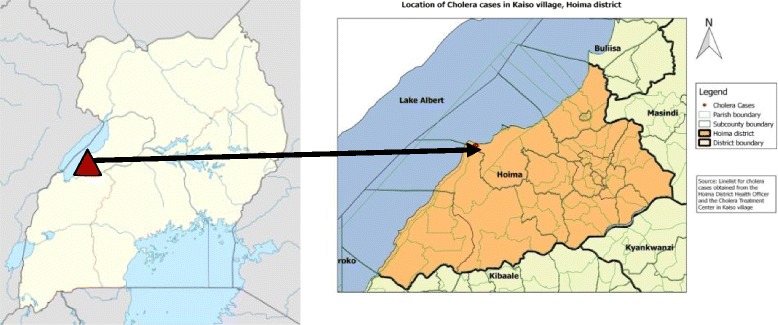
On 12 October 2015, a cholera outbreak involving 65 cases and two deaths was reported in a fishing village in Hoima District, Western Uganda. Despite initial response by the local health department, the outbreak persisted. We conducted an investigation to identify the source and mode of transmission, and recommend evidence-led interventions to control and prevent cholera outbreaks in this area.
We defined a suspected case as the onset of acute watery diarrhoea from 1 October to 2 November 2015 in a resident of Kaiso Village. A confirmed case was a suspected case who had Vibrio cholerae isolated from stool. We found cases by record review and active community case finding. We performed descriptive epidemiologic analysis for hypothesis generation. In an unmatched case-control study, we compared exposure histories of 61 cases and 126 controls randomly selected among asymptomatic village residents. We also conducted an environmental assessment and obtained meteorological data from a weather station.
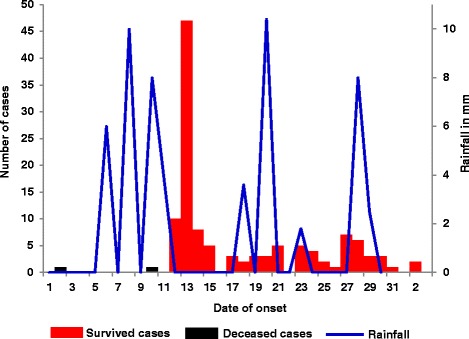
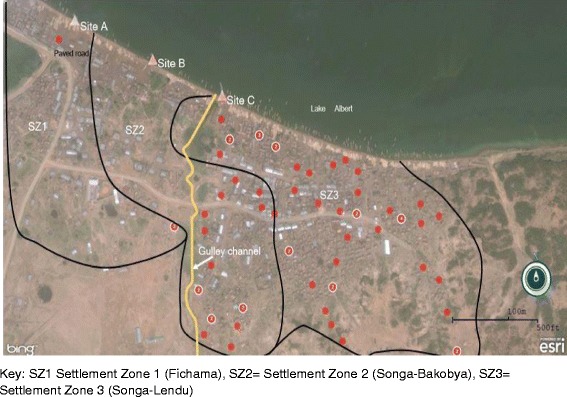
We identified 122 suspected cases, of which six were culture-confirmed, 47 were confirmed positive with a rapid diagnostic test and two died. The two deceased cases had onset of the disease on 2 October and 10 October, respectively. Heavy rainfall occurred on 7-11 October; a point-source outbreak occurred on 12-15 October, followed by continuous community transmission for two weeks. Village residents usually collected drinking water from three lakeshore points - A, B and C: 9.8% (6/61) of case-persons and 31% (39/126) of control-persons were found to usually use point A, 21% (13/61) of case-persons and 37% (46/126) of control-persons were found to usually use point B (OR = 1.8, 95% CI: 0.64-5.3), and 69% (42/61) of case-persons and 33% (41/126) of control-persons were found to usually use point C (OR = 6.7; 95% CI: 2.5-17) for water collection. All case-persons (61/61) and 93% (117/126) of control-persons reportedly never treated/boiled drinking water (OR = ∞, 95% CI : 1.0 - ∞). The village's piped water system had been vandalised and open defecation was common due to a lack of latrines. The lake water was found to be contiminated due to a gully channel that washed the faeces into the lake at point C.
This outbreak was likely caused by drinking lake water contaminated by faeces from a gully channel. We recommend treatment of drinking water, fixing the vandalised piped-water system and constructing latrines.
2015年10月12日,乌干达西部霍伊马区的一个渔村报告了一起霍乱疫情,涉及65例病例和2例死亡。尽管当地卫生部门做出了初步应对,但疫情仍在持续。我们开展了一项调查,以确定传染源和传播方式,并推荐以证据为导向的干预措施,以控制和预防该地区的霍乱疫情。
我们将2015年10月1日至11月2日期间凯索村居民出现急性水样腹泻定义为疑似病例。确诊病例是指粪便中分离出霍乱弧菌的疑似病例。我们通过记录审查和积极的社区病例发现来查找病例。我们进行描述性流行病学分析以生成假设。在一项非配对病例对照研究中,我们比较了61例病例和126名在无症状村民中随机选取的对照的暴露史。我们还进行了环境评估,并从一个气象站获取了气象数据。
我们确定了122例疑似病例,其中6例经培养确诊,47例快速诊断检测呈阳性,2例死亡。这两例死亡病例分别于10月2日和10月10日发病。10月7日至11日有暴雨;10月12日至15日发生了一次点源暴发,随后社区持续传播了两周。村民通常从三个湖岸取水点(A、B和C)收集饮用水:发现9.8%(6/61)的病例和31%(39/126)的对照通常使用取水点A,21%(13/61)的病例和37%(46/126)的对照通常使用取水点B(比值比[OR]=1.8,95%置信区间[CI]:0.64-5.3),69%(42/61)的病例和33%(41/126)的对照通常使用取水点C(OR=6.7;95%CI:2.5-17)取水。据报告,所有病例(61/61)和93%(117/126)的对照从未对饮用水进行处理/煮沸(OR=无穷大,95%CI:1.0-无穷大)。该村庄的自来水系统遭到破坏,由于缺乏厕所,露天排便很常见。发现湖水因一条沟渠被污染,该沟渠将粪便冲到了取水点C处的湖中。
此次疫情可能是由于饮用了被沟渠粪便污染的湖水所致。我们建议对饮用水进行处理,修复被破坏的自来水系统,并建造厕所。