Ouédraogo Samiratou, Ridde Valéry, Atchessi Nicole, Souares Aurélia, Koulidiati Jean-Louis, Stoeffler Quentin, Zunzunegui Maria-Victoria
University of Montreal Public Health Research Institute, Montreal, Canada.
Department of Social and Preventive Medicine, University of Montreal School of Public Health, Montreal, Canada.
BMJ Open. 2017 Oct 8;7(10):e013405. doi: 10.1136/bmjopen-2016-013405.
In Africa, health research on indigent people has focused on how to target them for services, but little research has been conducted to identify the social groups that compose indigence. Our aim was to identify what makes someone indigent beyond being recognised by the community as needing a card for free healthcare.
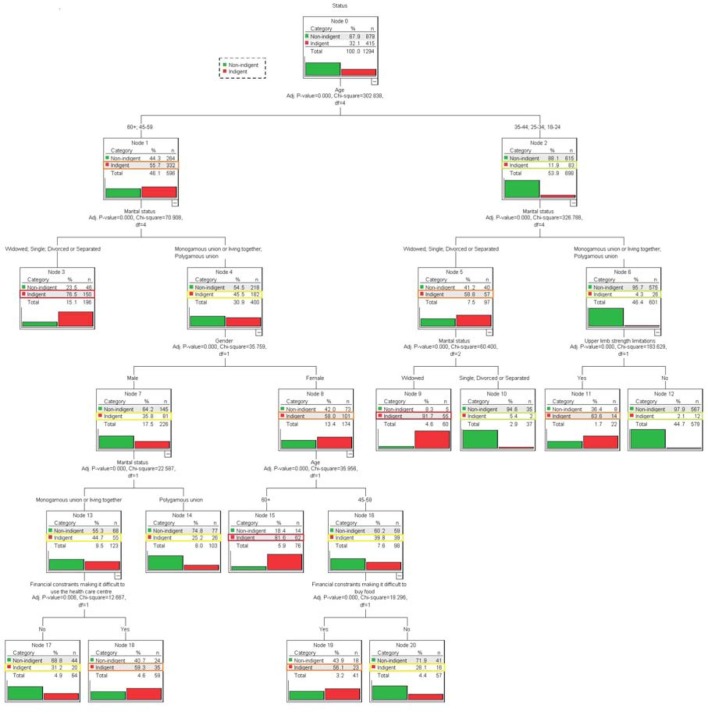
We used data from a survey conducted to evaluate a state-led intervention for performance-based financing of health services in two districts of Burkina Faso. In 2015, we analysed data of 1783 non-indigents and 829 people defined as indigents by their community in 21 villages following community-based targeting processes. Using a classification tree, we built a model to select socioeconomic and health characteristics that were likely to distinguish between non-indigents and indigents. We described the screening performance of the tree using data from specific nodes.
Widow(er)s under 45 years of age, unmarried people aged 45 years and over, and married women aged 60 years and over were more likely to be identified as indigents by their community. Simple rules based on age, marital status and gender detected indigents with sensitivity of 75.6% and specificity of 55% among those 45 years and over; among those under 45, sensitivity was 85.5% and specificity 92.2%. For both tests combined, sensitivity was 78% and specificity 81%.
In moving towards universal health coverage, Burkina Faso should extend free access to priority healthcare services to widow(er)s under 45, unmarried people aged 45 years and over, and married women aged 60 years and over, and services should be adapted to their health needs.
The collection, storage and release of data for research purposes were authorised by a government ethics committee in Burkina Faso (Decision No. 2013-7-066). Respondent consent was obtained verbally.
在非洲,针对贫困人口的健康研究主要集中在如何为他们提供服务,但对于构成贫困的社会群体的研究却很少。我们的目的是确定除了被社区认定需要免费医疗卡之外,还有哪些因素导致一个人陷入贫困。
我们使用了一项调查的数据,该调查旨在评估布基纳法索两个地区由国家主导的基于绩效的卫生服务筹资干预措施。2015年,我们分析了21个村庄中1783名非贫困人口和829名被社区定义为贫困人口的数据,这些数据是在基于社区的目标设定过程之后收集的。我们使用分类树构建了一个模型,以选择可能区分非贫困人口和贫困人口的社会经济和健康特征。我们使用来自特定节点的数据描述了该树的筛选性能。
45岁以下的寡妇/鳏夫、45岁及以上的未婚人士以及60岁及以上的已婚女性更有可能被社区认定为贫困人口。基于年龄、婚姻状况和性别的简单规则在45岁及以上人群中检测贫困人口的灵敏度为75.6%,特异度为55%;在45岁以下人群中,灵敏度为85.5%,特异度为92.2%。两项测试综合起来,灵敏度为78%,特异度为81%。
在迈向全民健康覆盖的过程中,布基纳法索应将优先医疗服务的免费获取范围扩大到45岁以下的寡妇/鳏夫、45岁及以上的未婚人士以及60岁及以上的已婚女性,并应根据他们的健康需求调整服务。
为研究目的收集、存储和发布数据已获得布基纳法索政府伦理委员会的批准(第2013-7-066号决定)。已口头获得受访者同意。