Valmy Larissa, Gontier Barbara, Parriault Marie Claire, Van Melle Astrid, Pavlovsky Thomas, Basurko Célia, Grenier Claire, Douine Maylis, Adenis Antoine, Nacher Mathieu
Centre d'Investigation Clinique Antilles-Guyane, Inserm 1424, Centre Hospitalier Andrée Rosemon, Av. des Flamboyants, 97306, Cayenne cedex, France.
Emergency Department, Centre Hospitalier Andrée Rosemon, Av. des Flamboyants, 97306, Cayenne cedex, France.
BMC Health Serv Res. 2016 Jan 28;16:34. doi: 10.1186/s12913-016-1284-y.
Access to health care is a global public problem. In French Guiana, there exists social inequalities which are specially marked amongst immigrants who make up a third of the population. Health care inequalities are prevalent. The objective of this study was to determine factors associated with why health care amongst the poor population of Cayenne was renounced. The study was cross sectional. It focused on knowledge, attitudes, practices and beliefs of the population living in poor neighborhoods of the Cayenne area.
Populations coming at the Red Cross mobile screening unit in poor urban areas of Cayenne were surveyed from July 2013 to June 2014. Structured questionnaires consisted of 93 questions. Written informed consent was requested at the beginning of the questionnaire. The predictors for renouncing medical care were determined using logistic regression models and tree analysis.
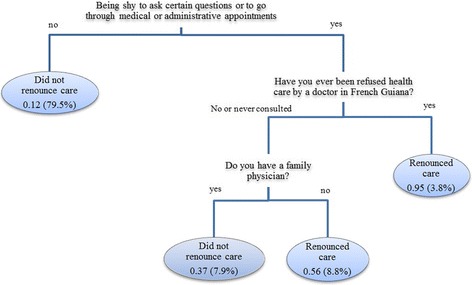
Twenty percent of persons had renounced care. Logistic regression showed that renouncement of health care was negatively associated with having no regular physician Adjusted Odds Ratio (AOR) = 0.43 (95 % CI = 0.24-0.79) and positively associated with being embarrassed to ask certain questions AOR = 6.81 (95 % CI = 3.98-11.65) and having been previously refused health care by a doctor AOR = 3.08 (95 % CI = 1.43-6.65). Tree analysis also showed that three of these variables were linked to renouncement, with feeling shy to ask certain questions as the first branching.
Although most people felt it was easy to see a doctor, one in five had renounced health care. The variables identified by the models suggest vulnerable persons generally had previous negative encounters with the health system and felt unwanted or non eligible for healthcare. Health care mediation and welcoming staff may be simple solutions to the above problems which were underscored in our observations.
获得医疗保健是一个全球性的公共问题。在法属圭亚那,社会不平等现象存在,在占人口三分之一的移民中尤为明显。医疗保健不平等现象普遍存在。本研究的目的是确定与卡宴贫困人口放弃医疗保健相关的因素。该研究为横断面研究。它关注卡宴地区贫困社区居民的知识、态度、行为和信仰。
2013年7月至2014年6月,对前往卡宴贫困城市地区红十字会流动筛查单位的人群进行了调查。结构化问卷由93个问题组成。在问卷开始时要求提供书面知情同意书。使用逻辑回归模型和树状分析确定放弃医疗护理的预测因素。
20%的人放弃了护理。逻辑回归显示,放弃医疗保健与没有固定医生呈负相关,调整后的优势比(AOR)=0.43(95%置信区间=0.24-0.79),与不好意思问某些问题呈正相关,AOR=6.81(95%置信区间=3.98-11.65),以及之前被医生拒绝医疗保健呈正相关,AOR=3.08(95%置信区间=1.43-6.65)。树状分析还表明,这些变量中的三个与放弃有关,其中不好意思问某些问题是第一个分支。
尽管大多数人认为看医生很容易,但五分之一的人放弃了医疗保健。模型确定的变量表明,弱势群体通常以前与医疗系统有过负面接触,并且觉得自己不受欢迎或没有资格获得医疗保健。医疗保健调解和热情的工作人员可能是解决上述我们观察中突出问题的简单办法。