Joshi Vidya Sagar, Kollu Sandeep S, Sharma Ram Murti
Department of Cardiac Anaesthesia, Military Hospital CTC, Pune, Maharashtra, India.
Department of Anaesthesiology and Critical Care, AFMC, Pune, Maharashtra, India.
Ann Card Anaesth. 2017 Oct-Dec;20(4):422-426. doi: 10.4103/aca.ACA_16_17.
The ideal anaesthetic technique for management of paediatric patients scheduled to undergo cardiac catheterisation is still not standardised.
To compare the effects of ketamine-propofol and ketamine-dexmedetomidine combinations on hemodynamic parameters and recovery time in paediatric patients undergoing minor procedures and cardiac catheterisation under sedation for various congenital heart diseases.
60 children of either sex undergoing cardiac catheterisation were randomly assigned into two groups Dexmedetomidine-ketamine group (DK) and Propofol-ketamine (PK) of 30 patients each. All patients were premedicated with glycopyrrolate and midazolam (0.05mg/kg) intravenously 5-10 min before anaesthetic induction. Group 'DK'received dexmedetomidineiv infusion 1 μg/kg over 10 min + ketamine1mg/kg bolus, followed by iv infusion of dexmedetomidine 0.5μg/kg/hr and of ketamine1 mg/kg/hr. Group 'PK' received propofol 1mg/kg and ketamine 1mg/kg/hr for induction followed by iv infusion of propofol 100 μg/kg/hr and ketamine 1 mg/kg/hr for maintenance. Haemodynamic parameters and recovery time was recorded postoperatively.
Independent sample t test was used to compare the statistical significance of continuous variables of both the groups.Chi square test was used for numerical data like gender.Fischer exact test was applied for non parametric data like ketamine consumption.
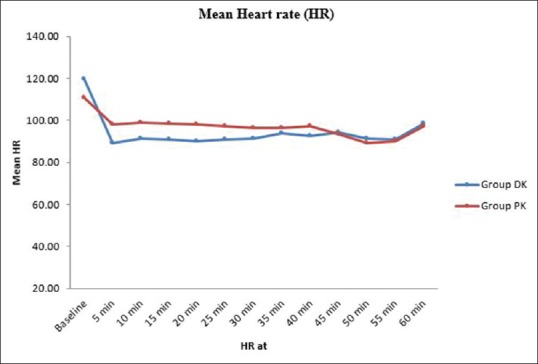
We observed that heart rate in dexmedetomidine (DK) group was significantly lower during the initial 25 mins after induction compared to the propofol (PK) group. Recovery was prolonged in the DK group compared to the PK group (40.88 vs. 22.28 min). Even ketamine boluses consumption was higher in DK group.
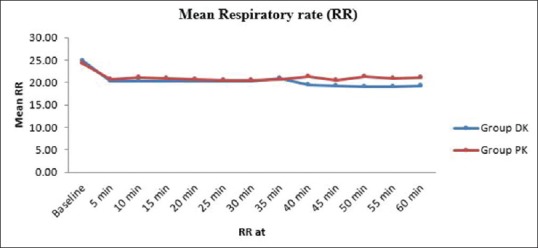
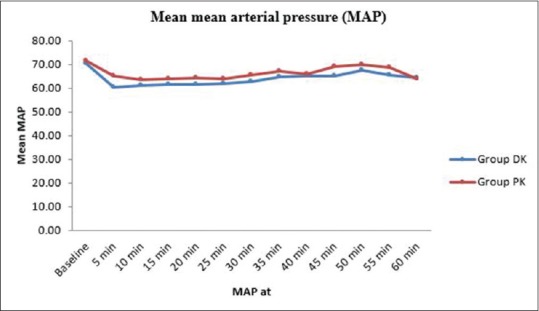
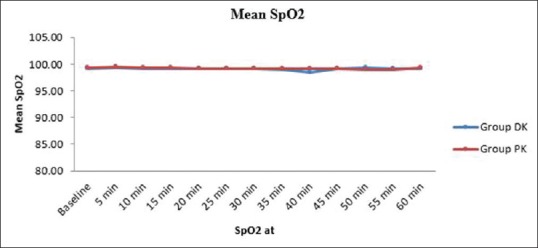
Use of dexmedetomidine-ketamine combination is a safe alternative, without any hemodynamic orrespiratory effects during the cardiac catheterization procedure but with some delayed recovery.
对于计划接受心导管插入术的儿科患者,理想的麻醉技术仍未标准化。
比较氯胺酮 - 丙泊酚和氯胺酮 - 右美托咪定组合对接受小型手术及因各种先天性心脏病在镇静下进行心导管插入术的儿科患者血流动力学参数和恢复时间的影响。
60例接受心导管插入术的儿童,随机分为两组,每组30例,右美托咪定 - 氯胺酮组(DK组)和丙泊酚 - 氯胺酮组(PK组)。所有患者在麻醉诱导前5 - 10分钟静脉注射格隆溴铵和咪达唑仑(0.05mg/kg)进行术前用药。“DK”组在10分钟内静脉输注右美托咪定1μg/kg + 氯胺酮1mg/kg推注,随后静脉输注右美托咪定0.5μg/kg/小时和氯胺酮1mg/kg/小时。“PK”组诱导时接受丙泊酚1mg/kg和氯胺酮1mg/kg/小时,随后静脉输注丙泊酚100μg/kg/小时和氯胺酮1mg/kg/小时维持。术后记录血流动力学参数和恢复时间。
采用独立样本t检验比较两组连续变量的统计学意义。卡方检验用于性别等数值数据。费舍尔精确检验用于氯胺酮消耗量等非参数数据。
我们观察到,与丙泊酚(PK)组相比,右美托咪定(DK)组诱导后最初25分钟内心率显著降低。与PK组相比,DK组恢复时间延长(40.88对22.28分钟)。甚至DK组氯胺酮推注量消耗也更高。
右美托咪定 - 氯胺酮组合是一种安全的替代方法,在心导管插入术过程中无任何血流动力学或呼吸影响,但恢复时间有所延迟。