Makita Kohzoh, Nishimoto Koshiro, Kiriyama-Kitamoto Kanako, Karashima Shigehiro, Seki Tsugio, Yasuda Masanori, Matsui Seishi, Omura Masao, Nishikawa Tetsuo
Department of Radiology, Nerima Hikarigaoka Hospital.
Department of Uro-Oncology, Saitama Medical University International Medical Center;
J Vis Exp. 2017 Sep 15(127):55716. doi: 10.3791/55716.
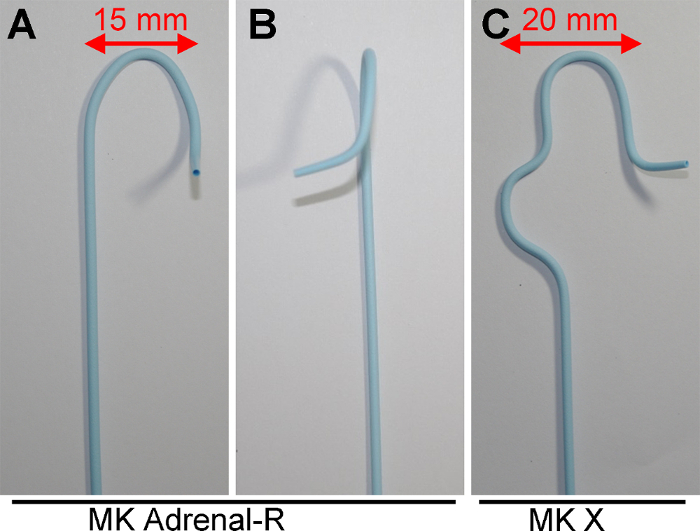
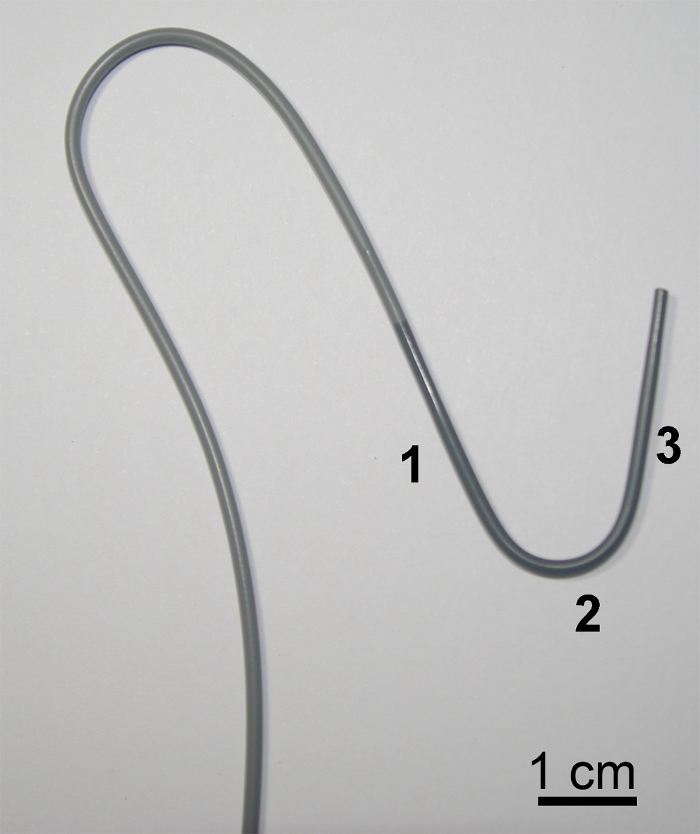
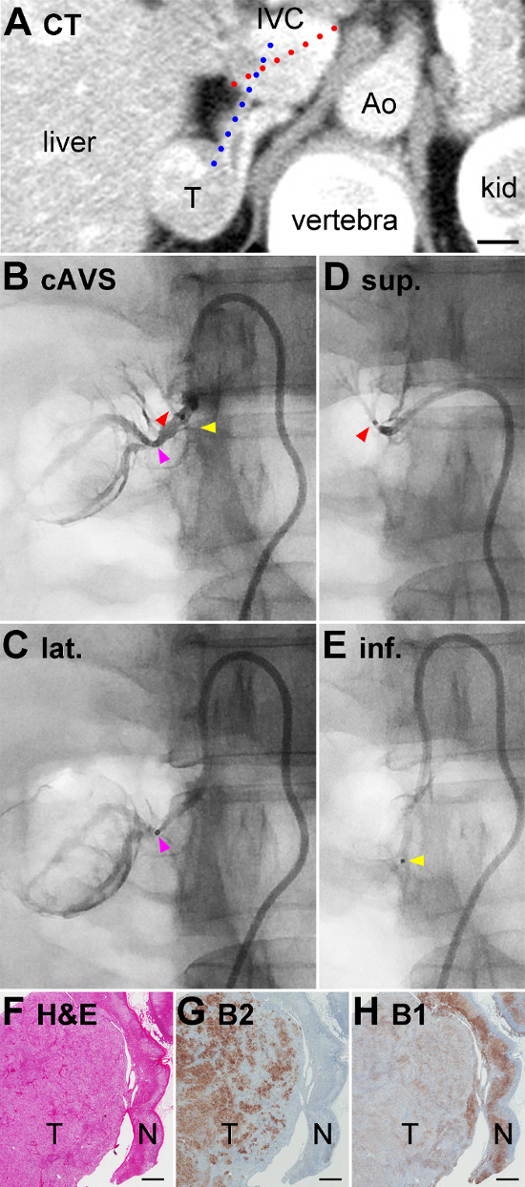
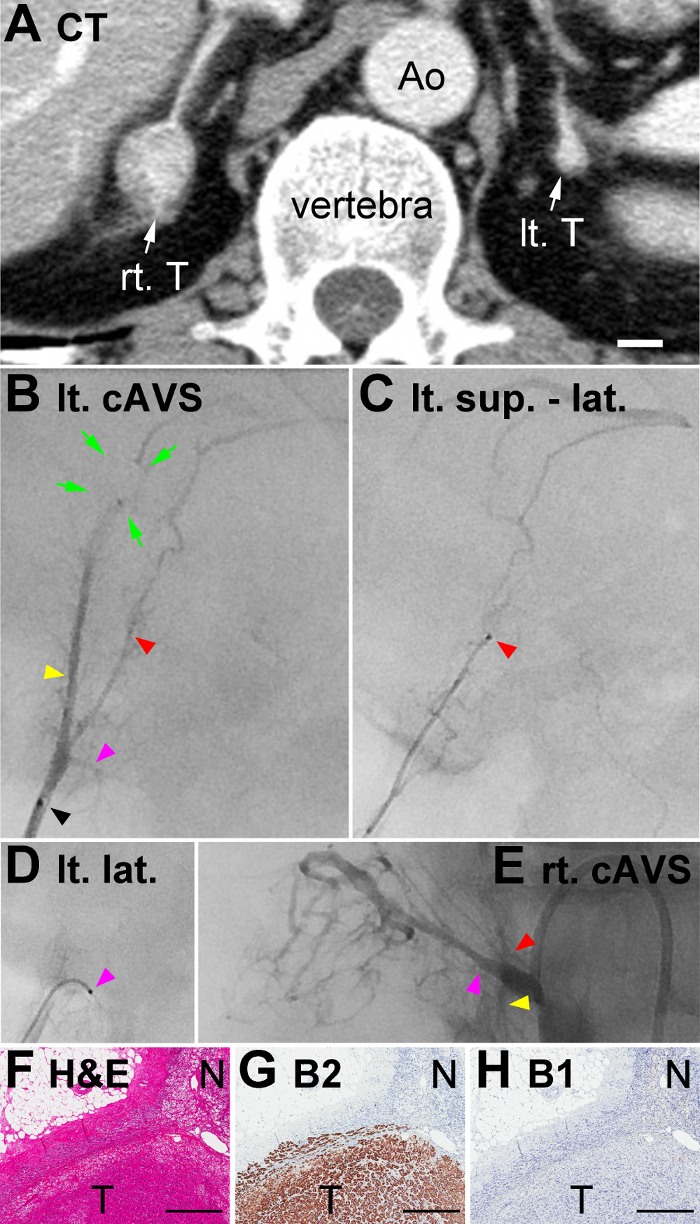
Primary aldosteronism (PA) and subclinical Cushing's syndrome (SCS) are conditions in which the adrenal glands autonomously produce excessive amounts of aldosterone and cortisol, respectively. The conventional adrenal venous sampling (cAVS) method collects blood samples from both adrenal central veins and is useful for identifying the laterality of excess hormone production in a unilateral lesion(s), as documented in PA cases. In cAVS, plasma cortisol concentrations (PCCs) are used to normalize plasma aldosterone concentrations (PACs). A novel "super-selective" adrenal venous sampling (ssAVS) method was developed using a micro-catheter, which collects blood samples from adrenal tributary veins (TVs). PACs in ssAVS samples do not require PCC normalization because samples contain a limited amount of systemic venous blood, if any. The ssAVS method enabled segmental lesion(s) to be detected in both adrenal glands, which may be treated by bilateral adrenalectomy, thereby sparing lesion-free segment(s). Right and left adrenals typically have three TVs each, i.e., the superior, lateral, and inferior TVs in the right adrenal as well as the superior-median, superior-lateral, and lateral TVs in the left adrenal. In the ssAVS method, specific parent catheters and a technique to handle them are required, and have been described herein. Furthermore, ssAVS results from three cases of PA are presented: bilateral aldosterone-producing adenoma (APA) (Case #1), left APA and right possible cortisol-producing adenoma causing SCS (Case #2), and idiopathic hyperaldosteronism in which bilateral adrenal segments produced excessive amounts of aldosterone (Case #3). The ssAVS method is not difficult for expert angiographers, and, thus, is recommended worldwide to treat PA cases for which cAVS does not represent a viable surgical treatment option.
原发性醛固酮增多症(PA)和亚临床库欣综合征(SCS)分别是肾上腺自主分泌过量醛固酮和皮质醇的病症。传统的肾上腺静脉采血(cAVS)方法从双侧肾上腺中央静脉采集血样,对于识别单侧病变中激素过量分泌的侧别很有用,如PA病例中所记录的那样。在cAVS中,血浆皮质醇浓度(PCC)用于标准化血浆醛固酮浓度(PAC)。一种使用微导管开发的新型“超选择性”肾上腺静脉采血(ssAVS)方法,从肾上腺属支静脉(TV)采集血样。ssAVS样本中的PAC不需要PCC标准化,因为样本中即使有也仅含有少量体循环静脉血。ssAVS方法能够检测到双侧肾上腺的节段性病变,这些病变可通过双侧肾上腺切除术治疗,从而保留无病变节段。右侧和左侧肾上腺通常各有三条TV,即右侧肾上腺的上、外侧和下TV,以及左侧肾上腺的上中、上外侧和外侧TV。在ssAVS方法中,需要特定的主导管及其操作技术,本文对此进行了描述。此外,还展示了3例PA患者的ssAVS结果:双侧醛固酮瘤(APA)(病例#1)、左侧APA和右侧可能导致SCS的皮质醇瘤(病例#2),以及双侧肾上腺节段分泌过量醛固酮的特发性醛固酮增多症(病例#3)。ssAVS方法对于专业血管造影师来说并不困难,因此,在全球范围内推荐用于治疗cAVS不适合作为可行手术治疗方案的PA病例。