Department of Neurosurgery, Beijing Tiantan Hospital, Capital Medical University, Beijing, China.
China National Clinical Research Center for Neurological Diseases (NCRC-ND), Beijing, China.
Stroke Vasc Neurol. 2017 Aug 24;2(3):140-146. doi: 10.1136/svn-2017-000089. eCollection 2017 Sep.
Few studies have reported the surgical treatment of carotid in-stent restenosis (ISR), more data and longer follow-up are needed. We describe the surgical treatment of ISR by standard carotid endarterectomy (CEA) with stent removal, including long-term follow-up in 10 patients from our centre.
Ten patients from our centre who underwent CEA with stent removal for ISR were retrospectively analysed, including nine symptomatic and one asymptomatic ISR of at least 70% with mean age 67.3, the median time between carotid artery stenting and CEA was 17 months (range, 2-54 months).
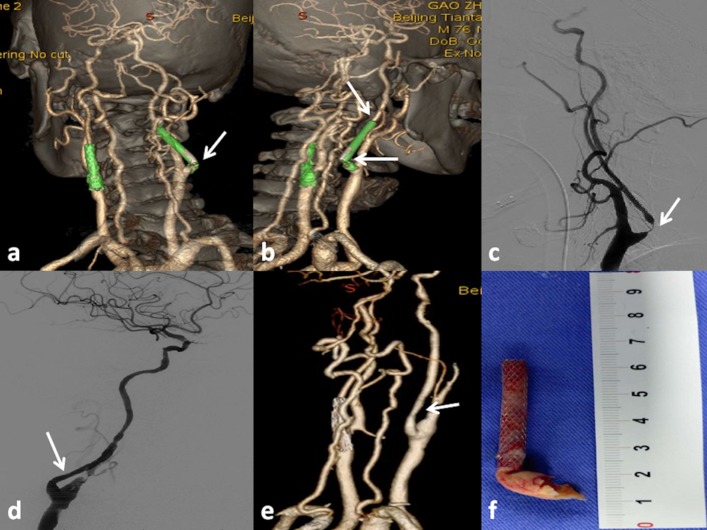
Standard CEA with stent removal was performed in all 10 patients without much technical difficulty (9 male and 1 female, mean age 67.3). Two cases were performed in hybrid operation room. There were a total of three complications that happened in three patients (30%) respectively. An asymptomatic dissecting aneurysm was formed on the petrous internal carotid artery in one patient who was followed up without intervention. In the second case, dissection occurred in the arterial wall distal to the site of the stent after stent removal revealed by intraoperative angiography, and another stent was implanted. The patient sustained temporary hypoglossal nerve dysfunction postoperatively. The third patient suffered cerebral hyperperfusion with complete recovery when discharged. No neurological complications occurred in other seven patients. After follow-up of 25 months (range, 11-54 months), one patient died of rectal cancer without ischaemic attack and restenosis 4 years postoperation; in one patient occurred recurrent symptomatic restenosis (90%) 1 year later; all other patients remained asymptomatic and without recurrent restenosis (>50%) by follow-up carotid ultrasound or CT angiography.
It seems that CEA with stent removal is a reasonable choice, by experienced hand, for symptomatic ISR with higher but acceptable complications. The indication of stent removal for asymptomatic ISR needs further observation.
很少有研究报道颈动脉支架内再狭窄(ISR)的手术治疗,需要更多的数据和更长时间的随访。我们描述了通过标准颈动脉内膜切除术(CEA)联合支架取出术治疗 ISR 的手术治疗方法,并报告了来自我们中心的 10 例患者的长期随访结果。
回顾性分析了我们中心 10 例行 CEA 联合支架取出术治疗 ISR 的患者,包括 9 例有症状和 1 例无症状的至少 70%狭窄的 ISR,平均年龄为 67.3 岁,颈动脉支架置入和 CEA 之间的中位时间为 17 个月(范围 2-54 个月)。
10 例患者均顺利完成标准 CEA 联合支架取出术(9 例男性,1 例女性,平均年龄 67.3)。2 例在杂交手术室进行。共有 3 例(30%)患者发生 3 种并发症。1 例患者在术后随访时发现无症状的岩骨内颈动脉夹层动脉瘤形成;第 2 例患者在术中血管造影显示支架取出后支架远端动脉壁夹层形成,再次植入支架;术后该患者出现暂时性舌下神经功能障碍。第 3 例患者出院时发生脑过度灌注,完全恢复。其他 7 例患者无神经并发症。随访 25 个月(范围 11-54 个月)后,1 例患者因直肠癌死亡,术后 4 年无缺血发作和再狭窄;1 例患者 1 年后发生复发性有症状再狭窄(90%);所有其他患者均无症状,通过随访颈动脉超声或 CT 血管造影无再狭窄(>50%)。
对于有症状的 ISR,经验丰富的术者采用 CEA 联合支架取出术似乎是一种合理的选择,虽然并发症发生率较高,但可接受。对于无症状的 ISR ,是否需要支架取出需要进一步观察。